

Red Eye: A Guide for Non-specialists
- PMID: 28530180
- PMCID: PMC5443986
- DOI: 10.3238/arztebl.2017.0302
Red Eye: A Guide for Non-specialists
Erratum in
-
Addenda.Dtsch Arztebl Int. 2017 Sep 22;114(38):641. doi: 10.3238/arztebl.2017.0641a. Dtsch Arztebl Int. 2017. PMID: 29017691 Free PMC article. No abstract available.
-
Erratum.Dtsch Arztebl Int. 2017 Jul;114(24):418. doi: 10.3238/arztebl.2017.0418. Epub 2017 Jul 16. Dtsch Arztebl Int. 2017. PMID: 31305768 Free PMC article.
Abstract
Background: Red eye can arise as a manifestation of many different systemic and ophthalmological diseases. The physician whom the patient first consults for this problem is often not an ophthalmologist. A correct assessment of the urgency of the situation is vitally important for the planning of further diagnostic evaluation and treatment.
Methods: This review is based on pertinent publications retrieved by a selective literature search in PubMed in August 2016 as well as on the authors' own clinical and scientific experience.
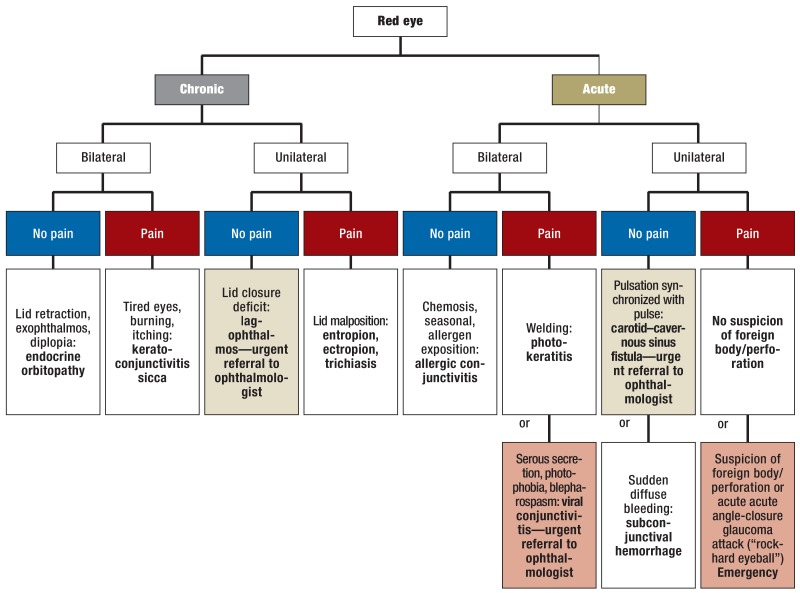
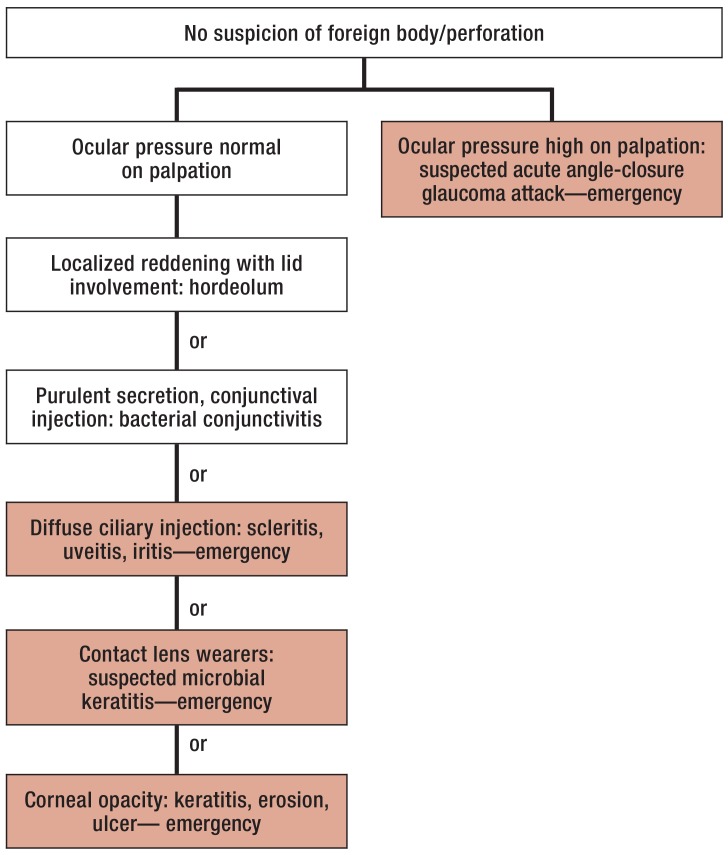
Results: Primary care physicians typically see 4-10 patients per week who complain of ocular symptoms. Most of them have red eye as the major clinical finding. A detailed history, baseline ophthalmological tests, and accompanying manifestations can narrow down the differential diagnosis. The duration and laterality of symptoms (uni- vs. bilateral) and the intensity of pain are the main criteria allowing the differentiation of non-critical changes that can be cared for by a general practitioner from diseases calling for elective referral to an ophthalmologist and eye emergencies requiring urgent ophthalmic surgery.
Conclusion: The differential diagnosis of red eye can be narrowed down rapidly with simple baseline tests and targeted questioning. Patients with ocular emergencies should be referred to an ophthalmologist at once, as should all patients whose diagnosis is in doubt.
Figures






Comment in
-
Misuse of Cortisone Eyedrops.Dtsch Arztebl Int. 2017 Sep 22;114(38):641. doi: 10.3238/arztebl.2017.0641b. Dtsch Arztebl Int. 2017. PMID: 29017692 Free PMC article. No abstract available.
-
Useful Pointers.Dtsch Arztebl Int. 2017 Sep 22;114(38):642. doi: 10.3238/arztebl.2017.0642a. Dtsch Arztebl Int. 2017. PMID: 29017693 Free PMC article. No abstract available.
References
-
- Pflipsen M, Massaquoi M, Wolf S. Evaluation of the painful eye. Am Fam Physician. 2016;93:991–998. - PubMed
-
- Cronau H, Kankanala RR, Mauger T. Diagnosis and management of red eye in primary care. Am Fam Physician. 2010;81:137–144. - PubMed
-
- Statham MO, Sharma A, Pane AR. Misdiagnosis of acute eye diseases by primary health care providers: incidence and implications. Med J Aust. 2008;189:402–404. - PubMed
-
- O‘Connor PM, Crock CT, Dhillon RS, Keeffe JE. Resources for the management of ocular emergencies in Australia. Emerg Med Australas. 2011;23:331–336. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical