

Vitamin A Status of Women and Children in Yaoundé and Douala, Cameroon, is Unchanged One Year after Initiation of a National Vitamin A Oil Fortification Program
- PMID: 28531099
- PMCID: PMC5452252
- DOI: 10.3390/nu9050522
Vitamin A Status of Women and Children in Yaoundé and Douala, Cameroon, is Unchanged One Year after Initiation of a National Vitamin A Oil Fortification Program
Abstract
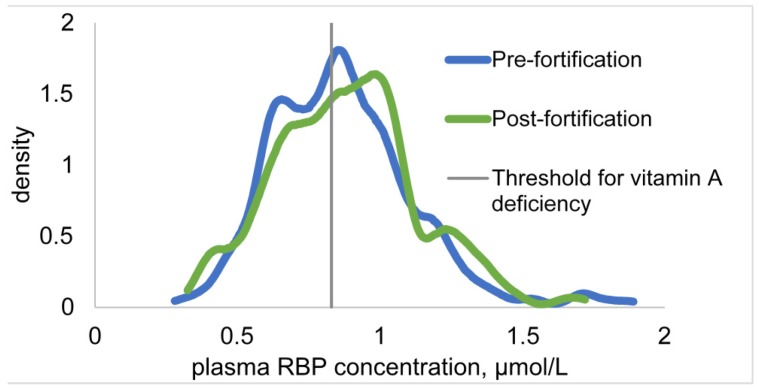
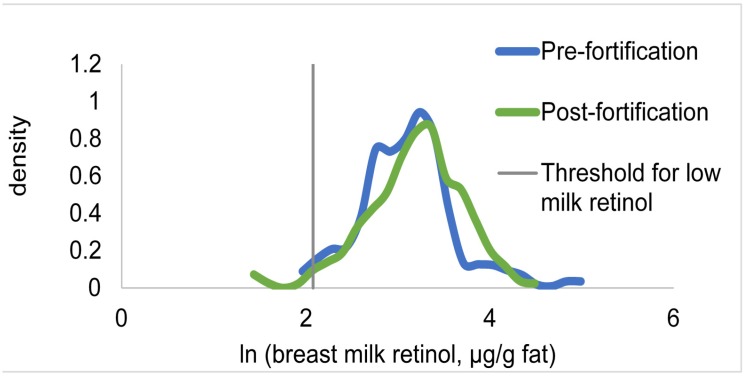
Vitamin A (VA) fortification of cooking oil is considered a cost-effective strategy for increasing VA status, but few large-scale programs have been evaluated. We conducted representative surveys in Yaoundé and Douala, Cameroon, 2 years before and 1 year after the introduction of a mandatory national program to fortify cooking oil with VA. In each survey, 10 different households were selected within each of the same 30 clusters (n = ~300). Malaria infection and plasma indicators of inflammation and VA (retinol-binding protein, pRBP) status were assessed among women aged 15-49 years and children aged 12-59 months, and casual breast milk samples were collected for VA and fat measurements. Refined oil intake was measured by a food frequency questionnaire, and VA was measured in household oil samples post-fortification. Pre-fortification, low inflammation-adjusted pRBP was common among children (33% <0.83 µmol/L), but not women (2% <0.78 µmol/L). Refined cooking oil was consumed by >80% of participants in the past week. Post-fortification, only 44% of oil samples were fortified, but fortified samples contained VA concentrations close to the target values. Controlling for age, inflammation, and other covariates, there was no difference in the mean pRBP, mean breast milk VA, prevalence of low pRBP, or prevalence of low milk VA between the pre- and post-fortification surveys. The frequency of refined oil intake was not associated with VA status indicators post-fortification. In sum, after a year of cooking oil fortification with VA, we did not detect evidence of increased plasma RBP or milk VA among urban women and preschool children, possibly because less than half of the refined oil was fortified. The enforcement of norms should be strengthened, and the program should be evaluated in other regions where the prevalence of VA deficiency was greater pre-fortification.
Keywords: breast milk; cooking oil; food fortification; retinol-binding protein; vitamin A.
Conflict of interest statement
This study was funded in part by a grant to R.E.S. and K.H.B. from Sight and Life, which is affiliated with DSM. The founding sponsors had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, and in the decision to publish the results. All other authors declare no conflict of interest.
Figures
References
-
- Stevens G., Bennett J., Hennocq Q., Lu Y., De-Regil L., Rogers L., Danaei G., Li G., White R., Flaxman S., et al. Trends and mortality effects of vitamin A deficiency in children in 138 low-income and middle-income countries between 1991 and 2013: A pooled analysis of population-based surveys. Lancet Glob. Health. 2015;3:e528–e536. doi: 10.1016/S2214-109X(15)00039-X. - DOI - PubMed
-
- Horton S., Alderman H., Rivera J.A. Copenhagen Consensus 2008 Challenge Paper. Copenhagen Consensus; Copenhagen, Denmark: 2008. The challenge of hunger and malnutrition.
-
- Arroyave G., Mejía L.A., Aguilar J.R. The effect of vitamin A fortification of sugar on the serum vitamin A levels of preschool Guatemalan children: A longitudinal evaluation. Am. J. Clin. Nutr. 1981;34:41–49. - PubMed
-
- Murdiana A., Azis I., Saidin S., Jahari A.B., Karyadi D. Vitamin A-fortified monosodium glutamate and vitamin A status: A controlled field trial. Am. J. Clin. Nutr. 1988;48:1265–1270. - PubMed
-
- Davila M., Norris L., Cleary M., Ross A. Vitamin A during lactation: Relationship of maternal diet to milk vitamin A content and to the vitamin A status of lactating rats and their pups. J. Nutr. 1985;115:1033–1041. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
