

Effect of Statin Treatment vs Usual Care on Primary Cardiovascular Prevention Among Older Adults: The ALLHAT-LLT Randomized Clinical Trial
- PMID: 28531241
- PMCID: PMC5543335
- DOI: 10.1001/jamainternmed.2017.1442
Effect of Statin Treatment vs Usual Care on Primary Cardiovascular Prevention Among Older Adults: The ALLHAT-LLT Randomized Clinical Trial
Abstract
Importance: While statin therapy for primary cardiovascular prevention has been associated with reductions in cardiovascular morbidity, the effect on all-cause mortality has been variable. There is little evidence to guide the use of statins for primary prevention in adults 75 years and older.
Objectives: To examine statin treatment among adults aged 65 to 74 years and 75 years and older when used for primary prevention in the Lipid-Lowering Trial (LLT) component of the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT-LLT).
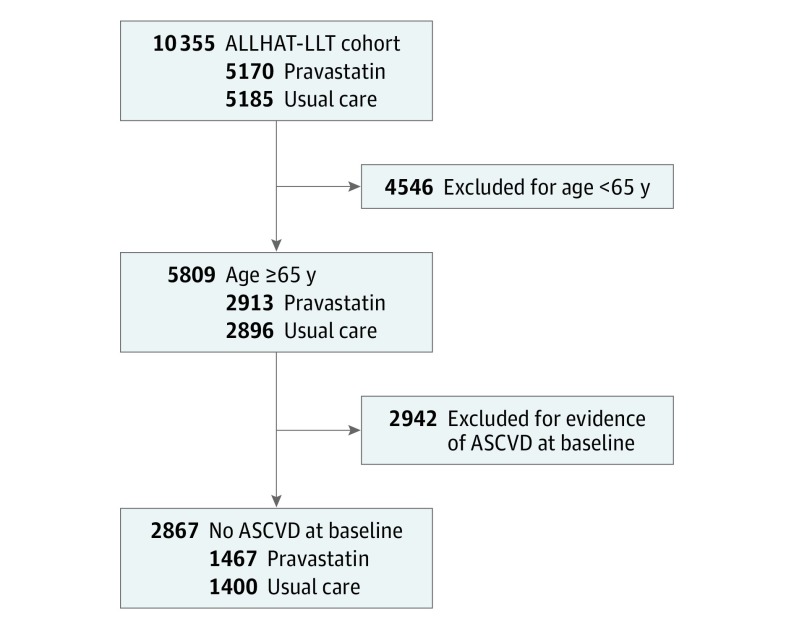
Design, setting, and participants: Post hoc secondary data analyses were conducted of participants 65 years and older without evidence of atherosclerotic cardiovascular disease; 2867 ambulatory adults with hypertension and without baseline atherosclerotic cardiovascular disease were included. The ALLHAT-LLT was conducted from February 1994 to March 2002 at 513 clinical sites.
Interventions: Pravastatin sodium (40 mg/d) vs usual care (UC).
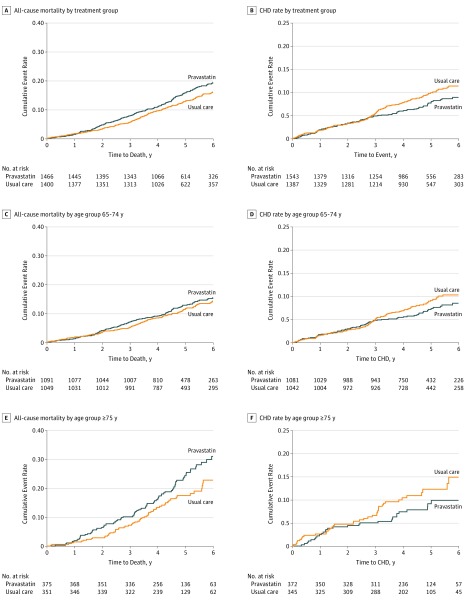
Main outcomes and measures: The primary outcome in the ALLHAT-LLT was all-cause mortality. Secondary outcomes included cause-specific mortality and nonfatal myocardial infarction or fatal coronary heart disease combined (coronary heart disease events).
Results: There were 1467 participants (mean [SD] age, 71.3 [5.2] years) in the pravastatin group (48.0% [n = 704] female) and 1400 participants (mean [SD] age, 71.2 [5.2] years) in the UC group (50.8% [n = 711] female). The baseline mean (SD) low-density lipoprotein cholesterol levels were 147.7 (19.8) mg/dL in the pravastatin group and 147.6 (19.4) mg/dL in the UC group; by year 6, the mean (SD) low-density lipoprotein cholesterol levels were 109.1 (35.4) mg/dL in the pravastatin group and 128.8 (27.5) mg/dL in the UC group. At year 6, of the participants assigned to pravastatin, 42 of 253 (16.6%) were not taking any statin; 71.0% in the UC group were not taking any statin. The hazard ratios for all-cause mortality in the pravastatin group vs the UC group were 1.18 (95% CI, 0.97-1.42; P = .09) for all adults 65 years and older, 1.08 (95% CI, 0.85-1.37; P = .55) for adults aged 65 to 74 years, and 1.34 (95% CI, 0.98-1.84; P = .07) for adults 75 years and older. Coronary heart disease event rates were not significantly different among the groups. In multivariable regression, the results remained nonsignificant, and there was no significant interaction between treatment group and age.
Conclusions and relevance: No benefit was found when pravastatin was given for primary prevention to older adults with moderate hyperlipidemia and hypertension, and a nonsignificant direction toward increased all-cause mortality with pravastatin was observed among adults 75 years and older.
Trial registration: clinicaltrials.gov Identifier: NCT00000542.
Conflict of interest statement
Figures
Comment in
-
Risks of Statin Therapy in Older Adults.JAMA Intern Med. 2017 Jul 1;177(7):966. doi: 10.1001/jamainternmed.2017.1457. JAMA Intern Med. 2017. PMID: 28531249 No abstract available.
-
Statine bringen in der Primärprävention ab 65 Jahren keinen Überlebensvorteil und sind potenziell schädlich.Praxis (Bern 1994). 2017 Aug;106(17):955-956. doi: 10.1024/1661-8157/a002765. Praxis (Bern 1994). 2017. PMID: 28830321 German. No abstract available.
References
-
- United States Census Bureau 2012 National population projections: summary tables. http://www.census.gov/population/projections/data/national/2012/summaryt.... Accessed April 10, 2017.
-
- Chokshi NP, Messerli FH, Sutin D, Supariwala AA, Shah NR. Appropriateness of statins in patients aged ≥80 years and comparison to other age groups. Am J Cardiol. 2012;110(10):1477-1481. - PubMed
-
- Johansen ME, Green LA. Statin use in very elderly individuals, 1999-2012. JAMA Intern Med. 2015;175(10):1715-1716. - PubMed
-
- Strandberg TE, Kolehmainen L, Vuorio A. Evaluation and treatment of older patients with hypercholesterolemia: a clinical review. JAMA. 2014;312(11):1136-1144. - PubMed
-
- Weinberger Y, Han BH. Statin treatment for older adults: the impact of the 2013 ACC/AHA cholesterol guidelines. Drugs Aging. 2015;32(2):87-93. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
