

Dual burden of malnutrition in US Affiliated Pacific jurisdictions in the Children's Healthy Living Program
- PMID: 28532446
- PMCID: PMC5440961
- DOI: 10.1186/s12889-017-4377-6
Dual burden of malnutrition in US Affiliated Pacific jurisdictions in the Children's Healthy Living Program
Abstract
Background: Few data are available on dual burden of under and over nutrition of children in the Pacific region. The objective was to examine prevalence of stunting at birth and current stunting and their relationship to obesity in US Affiliated Pacific (USAP) jurisdictions.
Methods: Cross sectional survey with cluster sampling by community. 5558, 2-8 years olds were measured in 51 communities in 11 USAP jurisdictions. The main outcome measures were stunting at birth, current stunting and obesity by body mass index. Prevalences of stunting at birth, current stunting and obesity were determined, adjusting for age distribution and community clustering. Differences by among age, sex, race and jurisdiction income levels were evaluated by chi-square analysis. Relationships of stunting at birth and current stunting with obesity were examined using a hierarchical model accounting for the study design.
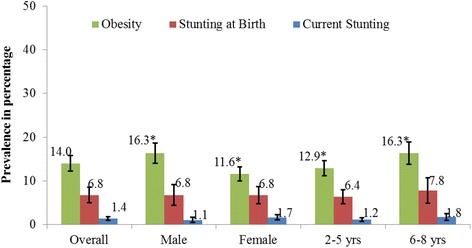
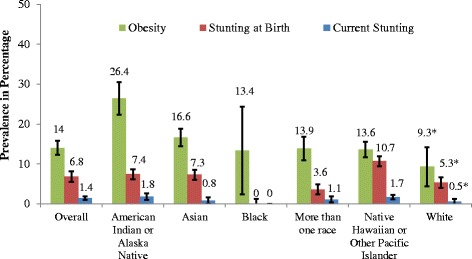
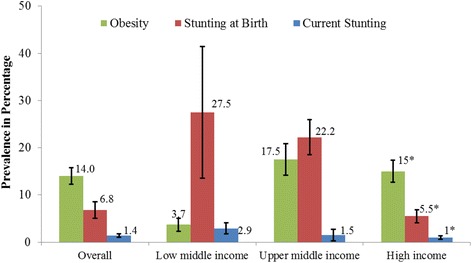
Results: Prevalences were stunting at birth 6.8% (Standard Error, SE = 0.9%), current stunting 1.4% (SE = 0.2%) and obesity 14.03.8% (SE = 0.9%). Obesity was highest in upper middle income jurisdictions (UMIJ) at 17.5%. Stunting at birth differed by race (p = 0.0001) with highest prevalence among Native Hawaiian/Pacific Islanders (10.7%). Prevalence of stunting at birth was different by jurisdiction income level with 27.5% in lower middle income jurisdictions (LMIJ), and 22.2% in UMIJ, and 5.5% in higher than high income jurisdictions (HIJ) at 5.5% (p < 0.0001). Prevalence of current stunting was higher in LMIJ than HIJ (p = 0.001), although children with current stunting were less likely to have been stunted at birth. The association between stunting at birth and current stunting was negative (OR = 0.19, 95% CI: 0.05-0.69).
Conclusions: Currently stunted children were marginally less likely to be obese than not stunted children in the USAP, where the prevalence of current stunting is low. Stunting (at birth and current) was highest in LMIJ, while UMIJ jurisdictions had the highest dual burden of malnutrition (that is the highest combination of both stunting at birth and obesity).
Trial registration: National Institutes for Health clinical trial # NCT01881373 (clinicaltrials.gov).
Keywords: Country; Income; Obesity; Pacific; Race; Stunting.
Figures
References
-
- Sawaya AL, Grillo LP, Verreschi I, da Silva AC, Roberts SB. Mild stunting is associated with higher susceptibility to the effects of high fat diets: studies in a shantytown population in Sao Paulo, Brazil. J Nutr. 1998;128(2 Suppl):415S–420S. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
