

Mechanical ventilation in idiopathic pulmonary fibrosis: a nationwide analysis of ventilator use, outcomes, and resource burden
- PMID: 28532459
- PMCID: PMC5441011
- DOI: 10.1186/s12890-017-0426-2
Mechanical ventilation in idiopathic pulmonary fibrosis: a nationwide analysis of ventilator use, outcomes, and resource burden
Abstract
Background: Idiopathic pulmonary fibrosis (IPF) is associated with increased risk of respiratory-related hospitalizations. Studies suggest mechanical ventilation (MV) use in IPF does not improve outcomes and guidelines recommend against its general use. Our objective was to investigate MV use and association with cost and mortality in IPF.
Methods: This retrospective study, using a nationwide sample, included claims with IPF (ICD-9-CM: 516.3) in 2009-2011 and principal respiratory disease diagnosis (ICD-9-CM: 460-519); excluding lung transplant. Regression models were used to determine predictors of MV and association with cost, LOS, and mortality. Domain analysis was used to account for use of subpopulation. Costs were adjusted to 2011. Data on patient severity not available.
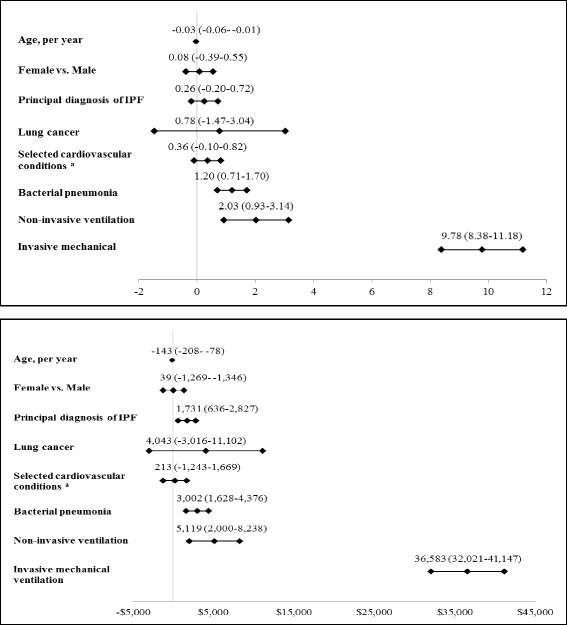
Results: Twenty two thousand three hundred fifty non-transplant IPF patients were admitted with principal respiratory disease diagnosis: Mean age 70.0 (SD 13.9), 49.1% female, mean LOS 7.4 (SD 8.2). MV was used in 11.4% of patients with a non-significant decline over time. In regression models, MV was associated with an increased stay of 9.78 days (95% CI 8.38-11.18) and increased cost of $36,583 (95% CI $32,021-41,147). MV users had significantly increased mortality (OR 15.55, 95% CI 12.13-19.95) versus nonusers.
Conclusions: Mechanical ventilation use has not significantly changed over time and is mostly used in younger patients and those admitted for non-IPF respiratory conditions. MV was associated with a 4-fold admission cost increase ($49,924 versus $11,742) and a 7-fold mortality increase (56% versus 7.5%), although patients who receive MV may differ from those who do not. Advances in treatment and decision aids are needed to improve outcomes in IPF.
Keywords: Cost of illness; Idiopathic pulmonary fibrosis; Mechanical ventilation; Mortality; Noninvasive ventilation; Outcomes.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
