

Multidimensional scaling of diffuse gliomas: application to the 2016 World Health Organization classification system with prognostically relevant molecular subtype discovery
- PMID: 28532485
- PMCID: PMC5439117
- DOI: 10.1186/s40478-017-0443-7
Multidimensional scaling of diffuse gliomas: application to the 2016 World Health Organization classification system with prognostically relevant molecular subtype discovery
Abstract
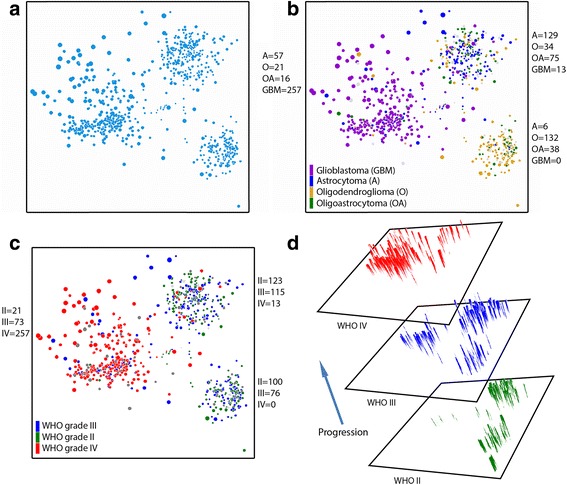
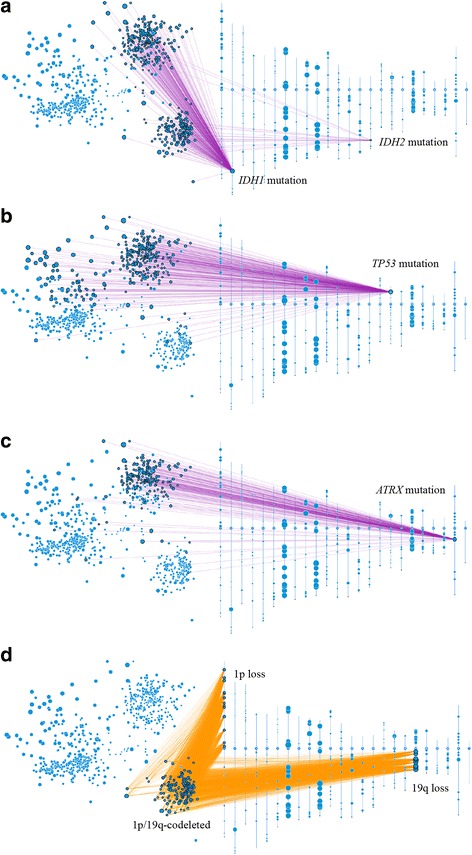
Recent updating of the World Health Organization (WHO) classification of central nervous system (CNS) tumors in 2016 demonstrates the first organized effort to restructure brain tumor classification by incorporating histomorphologic features with recurrent molecular alterations. Revised CNS tumor diagnostic criteria also attempt to reduce interobserver variability of histological interpretation and provide more accurate stratification related to clinical outcome. As an example, diffuse gliomas (WHO grades II-IV) are now molecularly stratified based upon isocitrate dehydrogenase 1 or 2 (IDH) mutational status, with gliomas of WHO grades II and III being substratified according to 1p/19q codeletion status. For now, grading of diffuse gliomas is still dependent upon histological parameters. Independent of WHO classification criteria, multidimensional scaling analysis of molecular signatures for diffuse gliomas from The Cancer Genome Atlas (TCGA) has identified distinct molecular subgroups, and allows for their visualization in 2-dimensional (2D) space. Using the web-based platform Oncoscape as a tool, we applied multidimensional scaling-derived molecular groups to the 2D visualization of the 2016 WHO classification of diffuse gliomas. Here we show that molecular multidimensional scaling of TCGA data provides 2D clustering that represents the 2016 WHO classification of diffuse gliomas. Additionally, we used this platform to successfully identify and define novel copy-number alteration-based molecular subtypes, which are independent of WHO grading, as well as predictive of clinical outcome. The prognostic utility of these molecular subtypes was further validated using an independent data set of the German Glioma Network prospective glioblastoma patient cohort.
Keywords: Astrocytoma; Glioblastoma; Glioma; Isocitrate Dehydrogenase (IDH); Oligodendroglioma; Oncoscape; World Health Organization (WHO).
Figures






References
-
- Bailey PCH. A classification of the tumours of the glioma group on a histogenetic basis with a correlated study of prognosis. City: J.B. Lippincott; 1926.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
