

The golden hour of acute ischemic stroke
- PMID: 28532498
- PMCID: PMC5440901
- DOI: 10.1186/s13049-017-0398-5
The golden hour of acute ischemic stroke
Abstract
Background: Acute Ischemic Stroke (AIS) treatment has been revolutionised in the last two decades with the increasing use of Intravenous Thrombolysis (IVT) and with the advent of Endovascular therapy (EVT). AIS treatment and outcome are time dependant and time saving measures are being implemented at every step of the treatment chain. These changes have resulted in lower treatment times in-hospital, but it is unclear if this translates into more patients being treated within 60 min of symptom onset - the Golden Hour. The clinical outcome of IVT therapy in this patient group was our secondary outcome.
Methods: From 2009 onwards, systematic changes were made to the AIS treatment chain leading to a dramatic decrease in Door-to-Needle (DTN) time. Analyses were performed on the number of these treatments year on year and their clinical outcomes within the Golden Hour at Stavanger University Hospital (SUS).
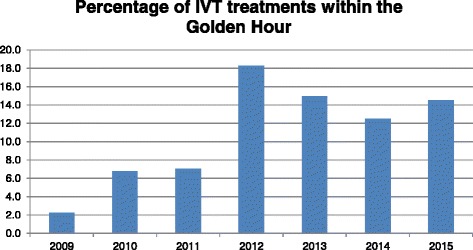
Results: Six-hundred and thirteen patients were included; seventy-three were treated within the Golden Hour. The percentage of total IVT treatments occurring in the Golden Hour rose from 2.2% in 2009 to 14.5% in 2015 (p = 0.006) with a high of 18.3% in 2012 (p < 0.001). All of these patients had a Median NIHSS of 0 at discharge, irrespective of age and pre-existing comorbidity. There was no incidence of any ICH and in-hospital mortality was only 2.7% in this group.
Discussion: The time from AIS symptom onset to treatment is filled with delays. Despite the inherence of some delays,significant efforts on the part of the pre- and in- hospital treatment chain have made IVT therapy within 60 min a possibility. The allocation and use of resources in the setting of rapid AIS treatment is warrantedand yields unprecedented results.
Conclusions: Our study shows that improved treatment routines led to an increase in the number of patients treated within the Golden Hour. Treatment in the Golden Hour leads to excellent outcomes in all patients, irrespective of age and pre-existing comorbidity.
Figures
References
-
- Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. N Engl J Med. 1995;333(24):1581-7. - PubMed
-
- Hacke W, et al. Randomised double-blind placebo-controlled trial of thrombolytic therapy with intravenous alteplase in acute ischaemic stroke (ECASS II). Second European-Australasian Acute Stroke Study Investigators. Lancet. 1998;352(9136):1245–1251. doi: 10.1016/S0140-6736(98)08020-9. - DOI - PubMed
-
- Molina CA, et al. REVASCAT: a randomized trial of revascularization with SOLITAIRE FR device vs. best medical therapy in the treatment of acute stroke due to anterior circulation large vessel occlusion presenting within eight-hours of symptom onset. Int J Stroke. 2015;10(4):619–626. doi: 10.1111/ijs.12157. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
