

Cardiovascular Toxicity of Illicit Anabolic-Androgenic Steroid Use
- PMID: 28533317
- PMCID: PMC5614517
- DOI: 10.1161/CIRCULATIONAHA.116.026945
Cardiovascular Toxicity of Illicit Anabolic-Androgenic Steroid Use
Abstract
Background: Millions of individuals have used illicit anabolic-androgenic steroids (AAS), but the long-term cardiovascular associations of these drugs remain incompletely understood.
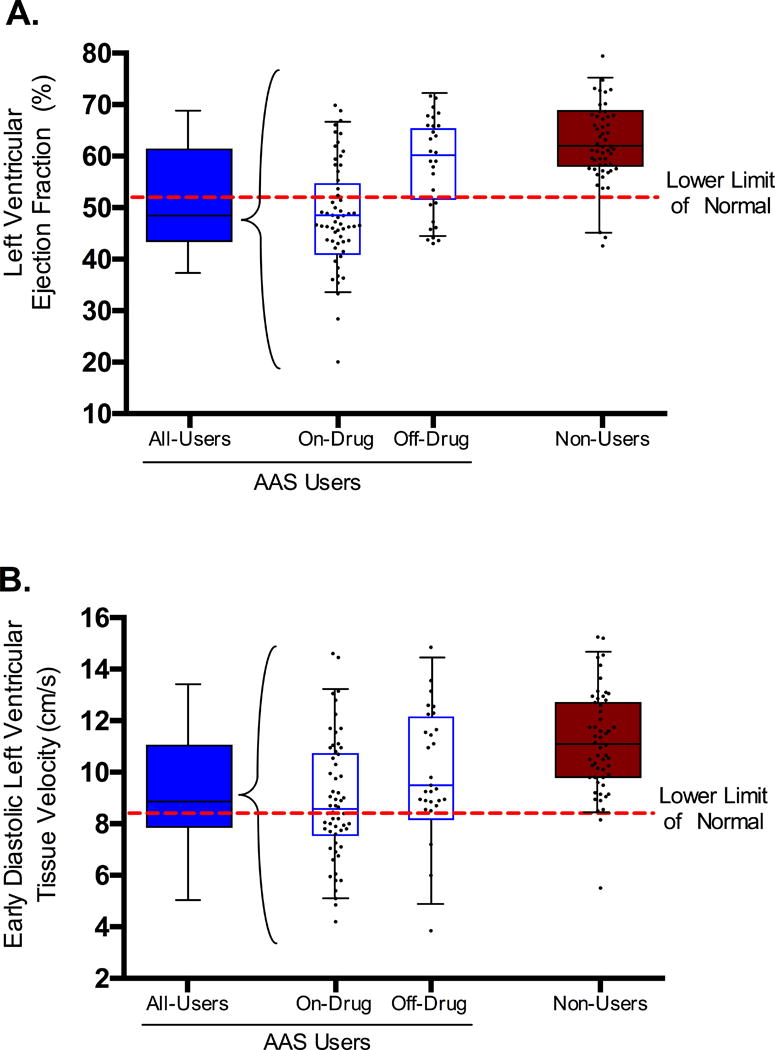
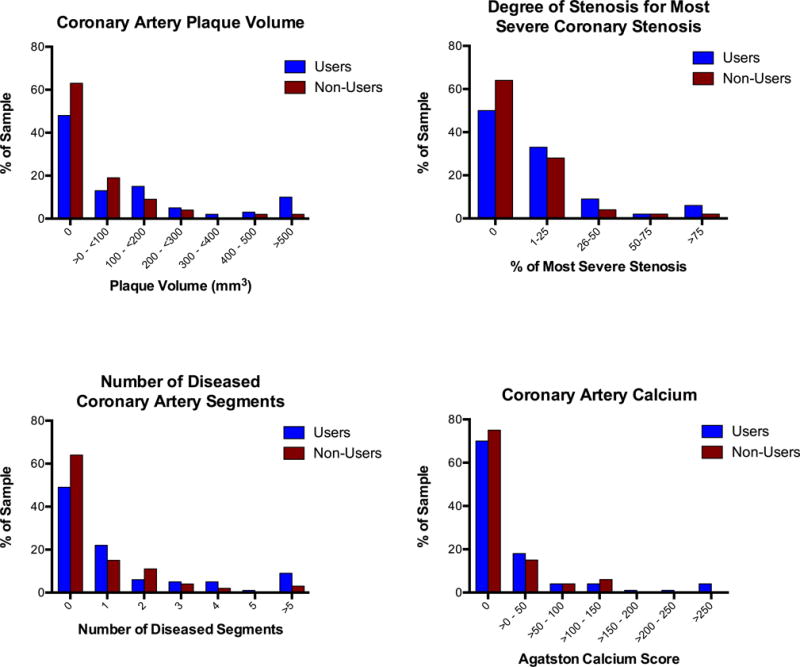
Methods: Using a cross-sectional cohort design, we recruited 140 experienced male weightlifters 34 to 54 years of age, comprising 86 men reporting ≥2 years of cumulative lifetime AAS use and 54 nonusing men. Using transthoracic echocardiography and coronary computed tomography angiography, we assessed 3 primary outcome measures: left ventricular (LV) systolic function (left ventricular ejection fraction), LV diastolic function (early relaxation velocity), and coronary atherosclerosis (coronary artery plaque volume).
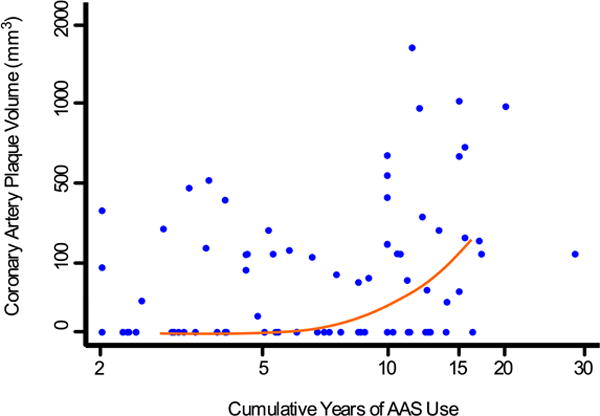
Results: Compared with nonusers, AAS users demonstrated relatively reduced LV systolic function (mean±SD left ventricular ejection fraction = 52±11% versus 63±8%; P<0.001) and diastolic function (early relaxation velocity = 9.3±2.4 cm/second versus 11.1±2.0 cm/second; P<0.001). Users currently taking AAS at the time of evaluation (N=58) showed significantly reduced LV systolic (left ventricular ejection fraction = 49±10% versus 58±10%; P<0.001) and diastolic function (early relaxation velocity = 8.9±2.4 cm/second versus 10.1±2.4 cm/second; P=0.035) compared with users currently off-drug (N=28). In addition, AAS users demonstrated higher coronary artery plaque volume than nonusers (median [interquartile range] 3 [0, 174] mL3 versus 0 [0, 69] mL3; P=0.012). Lifetime AAS dose was strongly associated with coronary atherosclerotic burden (increase [95% confidence interval] in rank of plaque volume for each 10-year increase in cumulative duration of AAS use: 0.60 SD units [0.16-1.03 SD units]; P=0.008).
Conclusions: Long-term AAS use appears to be associated with myocardial dysfunction and accelerated coronary atherosclerosis. These forms of AAS-associated adverse cardiovascular phenotypes may represent a previously underrecognized public-health problem.
Keywords: anabolic-androgenic steroids; atherosclerosis; cardiology; cardiomyopathy; diastolic dysfunction; men.
© 2017 American Heart Association, Inc.
Conflict of interest statement
Drs Kanayama and Weiner report no additional conflicts of interest. Dr Lu reports no conflicts of interest.
Figures
References
-
- McNutt RA, Ferenchick GS, Kirlin PC, Hamlin NJ. Acute myocardial infarction in a 22-year-old world class weight lifter using anabolic steroids. Am J Cardiol. 1988;62:164. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
