

Weekly Low-Dose Versus Three-Weekly High-Dose Cisplatin for Concurrent Chemoradiation in Locoregionally Advanced Non-Nasopharyngeal Head and Neck Cancer: A Systematic Review and Meta-Analysis of Aggregate Data
- PMID: 28533474
- PMCID: PMC5599190
- DOI: 10.1634/theoncologist.2017-0015
Weekly Low-Dose Versus Three-Weekly High-Dose Cisplatin for Concurrent Chemoradiation in Locoregionally Advanced Non-Nasopharyngeal Head and Neck Cancer: A Systematic Review and Meta-Analysis of Aggregate Data
Abstract
Background: Three-weekly high-dose cisplatin (100 mg/m2) is considered the standard systemic regimen given concurrently with postoperative or definitive radiotherapy in locally advanced squamous cell carcinoma of the head and neck (LA-SCCHN). However, due to unsatisfactory patient tolerance, various weekly low-dose schedules have been increasingly used in clinical practice. The aim of this meta-analysis was to compare the efficacy, safety, and compliance between these two approaches.
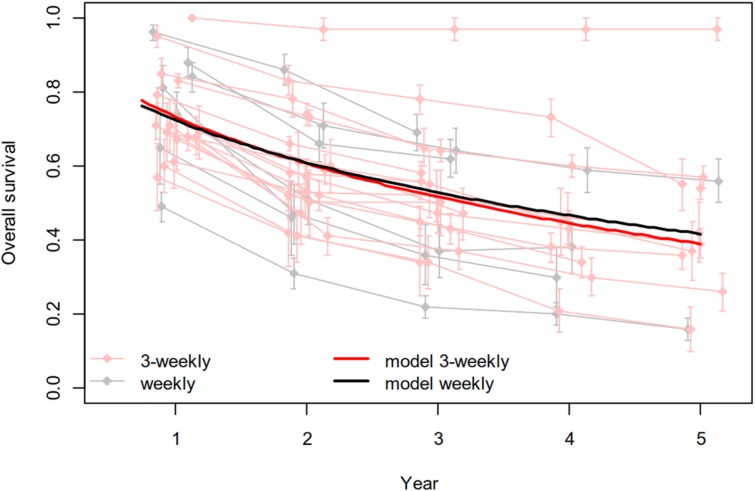
Materials and methods: We systematically searched literature for prospective trials of patients with LA-SCCHN who received postoperative or definitive conventionally fractionated concurrent chemoradiation. Radiation doses were usually 60-66 gray (Gy) in the postoperative setting and 66-70 Gy in the definitive setting. Standard, three-weekly high-dose cisplatin (100 mg/m2, 3 doses) was compared with the weekly low-dose protocol (≤50 mg/m2, ≥6 doses). The primary endpoint was overall survival. Secondary outcomes comprised response rate, acute and late adverse events, and treatment compliance.
Results: Fifty-two studies with 4,209 patients were included in two separate meta-analyses according to the two clinical settings. There was no difference in treatment efficacy as measured by overall survival or response rate between the chemoradiation settings with low-dose weekly and high-dose three-weekly cisplatin regimens. In the definitive treatment setting, the weekly regimen was more compliant and significantly less toxic with respect to severe (grade 3-4) myelosuppression (leukopenia p = .0083; neutropenia p = .0024), severe nausea and/or vomiting (p < .0001), and severe nephrotoxicity (p = .0099). Although in the postoperative setting the two approaches were more equal in compliance and with clearly less differences in the cisplatin-induced toxicities, the weekly approach induced more grade 3-4 dysphagia (p = .0026) and weight loss (p < .0001).
Conclusion: In LA-SCCHN, current evidence is insufficient to demonstrate a meaningful survival difference between the two dosing regimens. Prior to its adoption into routine clinical practice, the low-dose weekly approach needs to be prospectively compared with the standard three-weekly high-dose schedule.
Implications for practice: Given concurrently with conventional radiotherapy in locally advanced head and neck cancer, high-dose three-weekly cisplatin has often been replaced with weekly low-dose infusions to increase compliance and decrease toxicity. The present meta-analysis suggests that both approaches might be equal in efficacy, both in the definitive and postoperative settings, but differ in toxicity. However, some toxicity data can be influenced by unbalanced representation, and the conclusions are not based on adequately sized prospective randomized studies. Therefore, low-dose weekly cisplatin should not be used outside clinical trials but first prospectively studied in adequately sized phase III trials versus the high-dose three-weekly approach.
Keywords: Cisplatin; Head and neck cancer; Radiotherapy; Survival; Toxicity.
© AlphaMed Press 2017.
Conflict of interest statement
Disclosures of potential conflicts of interest may be found at the end of this article.
Figures


Comment in
-
Commentary on "Weekly Low-Dose Versus Three-Weekly High-Dose Cisplatin for Concurrent Chemoradiation in Locoregionally Advanced Non-Nasopharyngeal Head and Neck Cancer: A Systematic Review and Meta-Analysis of Aggregate Data".Oncologist. 2017 Sep;22(9):1022-1023. doi: 10.1634/theoncologist.2017-0232. Epub 2017 Jul 27. Oncologist. 2017. PMID: 28751507 Free PMC article.
References
-
- Adelstein DJ, Li Y, Adams GL et al. An intergroup phase III comparison of standard radiation therapy and two schedules of concurrent chemoradiotherapy in patients with unresectable squamous cell head and neck cancer. J Clin Oncol 2003;21:92–98. - PubMed
-
- Forastiere AA, Goepfert H, Maor M et al. Concurrent chemotherapy and radiotherapy for organ preservation in advanced laryngeal cancer. N Engl J Med 2003;349:2091–2098. - PubMed
-
- Bernier J, Domenge C, Ozsahin M et al. Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. N Engl J Med 2004;350:1945–1952. - PubMed
-
- Cooper JS, Pajak TF, Forastiere AA et al. Postoperative concurrent radiotherapy and chemotherapy for high‐risk squamous‐cell carcinoma of the head and neck. N Engl J Med 2004;350:1937–1944. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
