

Renal dysfunction in cirrhosis: acute kidney injury and the hepatorenal syndrome
- PMID: 28533910
- PMCID: PMC5421450
- DOI: 10.1093/gastro/gox009
Renal dysfunction in cirrhosis: acute kidney injury and the hepatorenal syndrome
Abstract
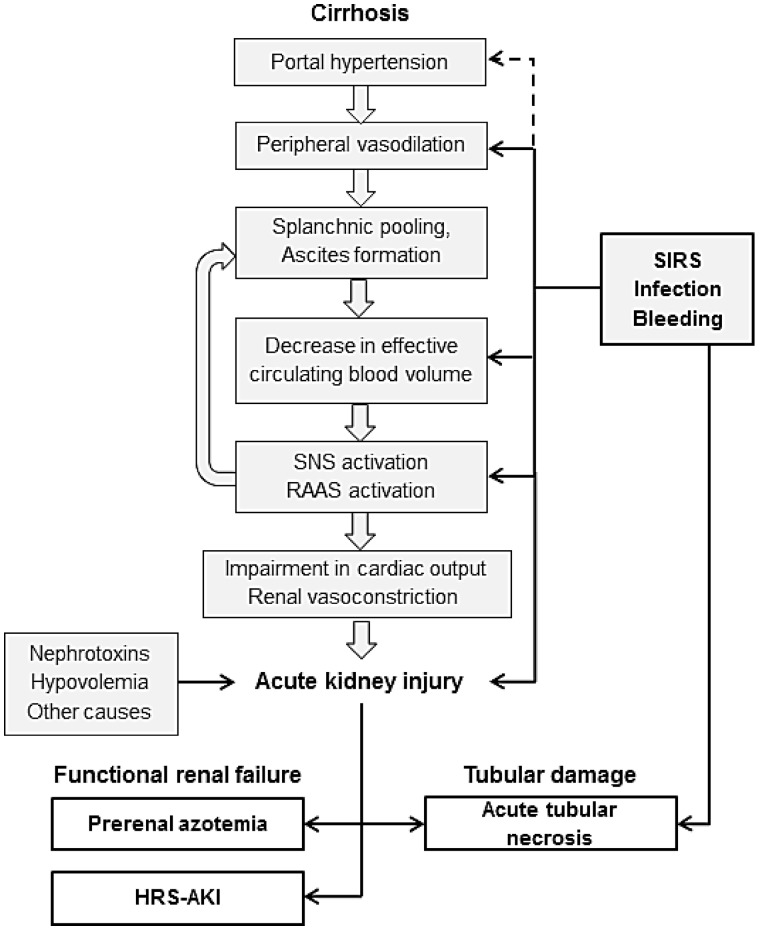
Renal dysfunction is a common complication of liver cirrhosis and of utmost clinical and prognostic relevance. Patients with cirrhosis are more prone to developing acute kidney injury (AKI) than the non-cirrhotic population. Pre-renal AKI, the hepatorenal syndrome type of AKI (HRS-AKI, formerly known as 'type 1') and acute tubular necrosis represent the most common causes of AKI in cirrhosis. Correct differentiation is imperative, as treatment differs substantially. While pre-renal AKI usually responds well to plasma volume expansion, HRS-AKI and ATN require different specific approaches and are associated with substantial mortality. Several paradigms, such as the threshold of 2.5 mg/dL for diagnosis of HRS-AKI, have recently been abolished and novel urinary biomarkers are being investigated in order to facilitate early and correct diagnosis and treatment of HRS-AKI and other forms of AKI in patients with cirrhosis. This review summarizes the current diagnostic criteria, as well as pathophysiologic and therapeutic concepts for AKI and HRS-AKI in cirrhosis.
Keywords: acute kidney injury; hepatorenal syndrome; liver cirrhosis.
Figures
References
-
- Alessandria C, Ozdogan O, Guevara M. et al. MELD score and clinical type predict prognosis in hepatorenal syndrome: relevance to liver transplantation. Hepatology 2005;41: 1282–9. - PubMed
-
- Nair S, Verma S, Thuluvath PJ.. Pretransplant renal function predicts survival in patients undergoing orthotopic liver transplantation. Hepatology 2002;35:1179–85. - PubMed
-
- Wiesner R, Edwards E, Freeman R. et al. Model for end-stage liver disease (MELD) and allocation of donor livers. Gastroenterology 2003;124:91–6. - PubMed
-
- Wong F. Recent advances in our understanding of hepatorenal syndrome. Nat Rev Gastroenterol Hepatol 2012;9:382–91. - PubMed
-
- Gerbes AL. Liver cirrhosis and kidney. Dig Dis 2016;34:387–90. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
