

Unravelling the biology of SCLC: implications for therapy
- PMID: 28534531
- PMCID: PMC5843484
- DOI: 10.1038/nrclinonc.2017.71
Unravelling the biology of SCLC: implications for therapy
Abstract
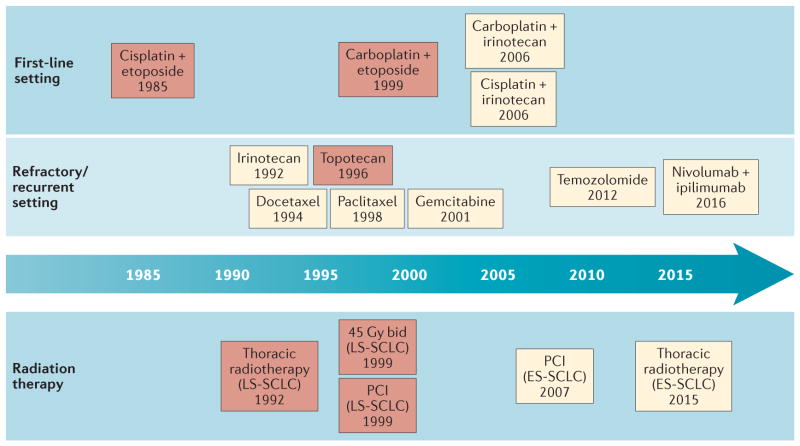
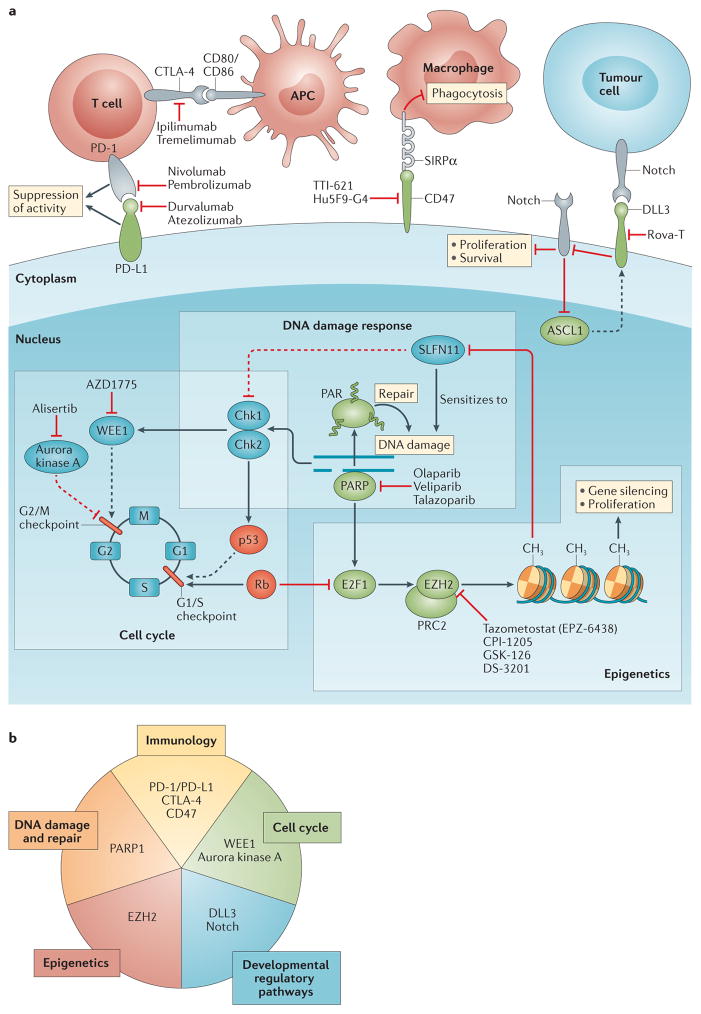
Small-cell lung cancer (SCLC) is an aggressive malignancy associated with a poor prognosis. First-line treatment has remained unchanged for decades, and a paucity of effective treatment options exists for recurrent disease. Nonetheless, advances in our understanding of SCLC biology have led to the development of novel experimental therapies. Poly [ADP-ribose] polymerase (PARP) inhibitors have shown promise in preclinical models, and are under clinical investigation in combination with cytotoxic therapies and inhibitors of cell-cycle checkpoints.Preclinical data indicate that targeting of histone-lysine N-methyltransferase EZH2, a regulator of chromatin remodelling implicated in acquired therapeutic resistance, might augment and prolong chemotherapy responses. High expression of the inhibitory Notch ligand Delta-like protein 3 (DLL3) in most SCLCs has been linked to expression of Achaete-scute homologue 1 (ASCL1; also known as ASH-1), a key transcription factor driving SCLC oncogenesis; encouraging preclinical and clinical activity has been demonstrated for an anti-DLL3-antibody-drug conjugate. The immune microenvironment of SCLC seems to be distinct from that of other solid tumours, with few tumour-infiltrating lymphocytes and low levels of the immune-checkpoint protein programmed cell death 1 ligand 1 (PD-L1). Nonetheless, immunotherapy with immune-checkpoint inhibitors holds promise for patients with this disease, independent of PD-L1 status. Herein, we review the progress made in uncovering aspects of the biology of SCLC and its microenvironment that are defining new therapeutic strategies and offering renewed hope for patients.
Conflict of interest statement
C.M.R. has been a paid consultant regarding oncology drug development for Bristol Myers Squibb, Celgene, G1 Therapeutics, Harpoon Therapeutics, Medivation, and Novartis. The other authors declare no competing interests.
Figures
References
-
- Ferlay J, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136:E359–E386. - PubMed
-
- Torre LA, et al. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65:87–108. - PubMed
-
- Nicholson AG, et al. The International Association for the Study of Lung Cancer Lung Cancer staging project: proposals for the revision of the clinical and pathologic staging of small cell lung cancer in the forthcoming eighth edition of the TNM classification for lung cancer. J Thorac Oncol. 2016;11:300–311. - PubMed
-
- Jemal A, et al. Cancer Statistics, 2007. CA Cancer J Clin. 2007;57:43–66. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
