

Effect of Cephalexin Plus Trimethoprim-Sulfamethoxazole vs Cephalexin Alone on Clinical Cure of Uncomplicated Cellulitis: A Randomized Clinical Trial
- PMID: 28535235
- PMCID: PMC5815038
- DOI: 10.1001/jama.2017.5653
Effect of Cephalexin Plus Trimethoprim-Sulfamethoxazole vs Cephalexin Alone on Clinical Cure of Uncomplicated Cellulitis: A Randomized Clinical Trial
Abstract
Importance: Emergency department visits for skin infections in the United States have increased with the emergence of methicillin-resistant Staphylococcus aureus (MRSA). For cellulitis without purulent drainage, β-hemolytic streptococci are presumed to be the predominant pathogens. It is unknown if antimicrobial regimens possessing in vitro MRSA activity provide improved outcomes compared with treatments lacking MRSA activity.
Objective: To determine whether cephalexin plus trimethoprim-sulfamethoxazole yields a higher clinical cure rate of uncomplicated cellulitis than cephalexin alone.
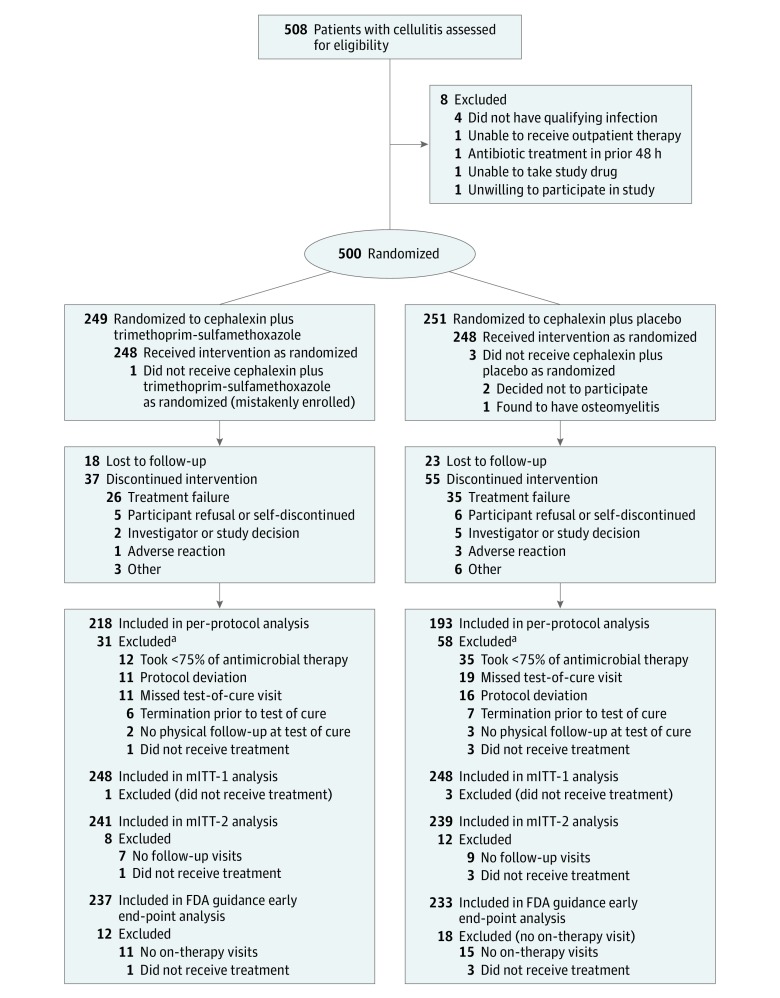
Design, setting, and participants: Multicenter, double-blind, randomized superiority trial in 5 US emergency departments among outpatients older than 12 years with cellulitis and no wound, purulent drainage, or abscess enrolled from April 2009 through June 2012. All participants had soft tissue ultrasound performed at the time of enrollment to exclude abscess. Final follow-up was August 2012.
Interventions: Cephalexin, 500 mg 4 times daily, plus trimethoprim-sulfamethoxazole, 320 mg/1600 mg twice daily, for 7 days (n = 248 participants) or cephalexin plus placebo for 7 days (n = 248 participants).
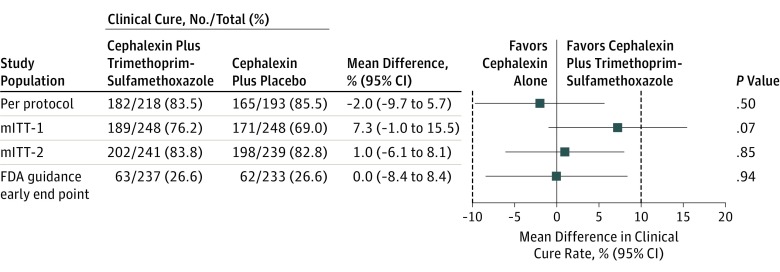
Main outcomes and measures: The primary outcome determined a priori in the per-protocol group was clinical cure, defined as absence of these clinical failure criteria at follow-up visits: fever; increase in erythema (>25%), swelling, or tenderness (days 3-4); no decrease in erythema, swelling, or tenderness (days 8-10); and more than minimal erythema, swelling, or tenderness (days 14-21). A clinically significant difference was defined as greater than 10%.
Results: Among 500 randomized participants, 496 (99%) were included in the modified intention-to-treat analysis and 411 (82.2%) in the per-protocol analysis (median age, 40 years [range, 15-78 years]; 58.4% male; 10.9% had diabetes). Median length and width of erythema were 13.0 cm and 10.0 cm. In the per-protocol population, clinical cure occurred in 182 (83.5%) of 218 participants in the cephalexin plus trimethoprim-sulfamethoxazole group vs 165 (85.5%) of 193 in the cephalexin group (difference, -2.0%; 95% CI, -9.7% to 5.7%; P = .50). In the modified intention-to-treat population, clinical cure occurred in 189 (76.2%) of 248 participants in the cephalexin plus trimethoprim-sulfamethoxazole group vs 171 (69.0%) of 248 in the cephalexin group (difference, 7.3%; 95% CI, -1.0% to 15.5%; P = .07). Between-group adverse event rates and secondary outcomes through 7 to 9 weeks, including overnight hospitalization, recurrent skin infections, and similar infection in household contacts, did not differ significantly.
Conclusions and relevance: Among patients with uncomplicated cellulitis, the use of cephalexin plus trimethoprim-sulfamethoxazole compared to cephalexin alone did not result in higher rates of clinical resolution of cellulitis in the per-protocol analysis. However, because imprecision around the findings in the modified intention-to-treat analysis included a clinically important difference favoring cephalexin plus trimethoprim-sulfamethoxazole, further research may be needed.
Trial registration: clinicaltrials.gov Identifier: NCT00729937.
Conflict of interest statement
Figures
Comment in
-
Empirical MRSA Coverage for Nonpurulent Cellulitis: Swinging the Pendulum Away From Routine Use.JAMA. 2017 May 23;317(20):2070-2071. doi: 10.1001/jama.2017.5654. JAMA. 2017. PMID: 28535215 No abstract available.
-
Ein unkompliziertes Erysipel kann weiterhin mit nur einem Antibiotikum behandelt werden.Praxis (Bern 1994). 2017 Aug;106(17):957-958. doi: 10.1024/1661-8157/a002764. Praxis (Bern 1994). 2017. PMID: 28830322 German. No abstract available.
-
Adding trimethoprim-sulfamethoxazole to cephalexin did not increase clinical cure in uncomplicated cellulitis.Ann Intern Med. 2017 Oct 17;167(8):JC40. doi: 10.7326/ACPJC-2017-167-8-040. Ann Intern Med. 2017. PMID: 29049759 No abstract available.
-
Cephalexin plus trimethoprim-sulfamethoxazole was not superior to cephalexin alone for the treatment of outpatient non-purulent cellulitis.Evid Based Med. 2017 Dec;22(6):213. doi: 10.1136/ebmed-2017-110796. Epub 2017 Nov 10. Evid Based Med. 2017. PMID: 29127212 No abstract available.
Similar articles
-
Clinical trial: comparative effectiveness of cephalexin plus trimethoprim-sulfamethoxazole versus cephalexin alone for treatment of uncomplicated cellulitis: a randomized controlled trial.Clin Infect Dis. 2013 Jun;56(12):1754-62. doi: 10.1093/cid/cit122. Epub 2013 Mar 1. Clin Infect Dis. 2013. PMID: 23457080 Clinical Trial.
-
Trimethoprim-Sulfamethoxazole versus Placebo for Uncomplicated Skin Abscess.N Engl J Med. 2016 Mar 3;374(9):823-32. doi: 10.1056/NEJMoa1507476. N Engl J Med. 2016. PMID: 26962903 Free PMC article. Clinical Trial.
-
A Randomized Trial of Clindamycin Versus Trimethoprim-sulfamethoxazole for Uncomplicated Wound Infection.Clin Infect Dis. 2016 Jun 15;62(12):1505-1513. doi: 10.1093/cid/ciw177. Epub 2016 Mar 29. Clin Infect Dis. 2016. PMID: 27025829 Free PMC article. Clinical Trial.
-
Cellulitis: A Review of Current Practice Guidelines and Differentiation from Pseudocellulitis.Am J Clin Dermatol. 2022 Mar;23(2):153-165. doi: 10.1007/s40257-021-00659-8. Epub 2021 Dec 13. Am J Clin Dermatol. 2022. PMID: 34902109 Review.
-
Antibacterials as adjuncts to incision and drainage for adults with purulent methicillin-resistant Staphylococcus aureus (MRSA) skin infections.Drugs. 2012 Feb 12;72(3):339-51. doi: 10.2165/11599510-000000000-00000. Drugs. 2012. PMID: 22316350 Review.
Cited by
-
Is coverage of S. aureus necessary in cellulitis/erysipelas? A literature review.Infection. 2020 Apr;48(2):183-191. doi: 10.1007/s15010-019-01382-7. Epub 2019 Dec 16. Infection. 2020. PMID: 31845187
-
A Multicenter Evaluation of Vancomycin-Associated Acute Kidney Injury in Hospitalized Patients with Acute Bacterial Skin and Skin Structure Infections.Infect Dis Ther. 2020 Mar;9(1):89-106. doi: 10.1007/s40121-019-00278-1. Epub 2020 Jan 25. Infect Dis Ther. 2020. PMID: 31983021 Free PMC article.
-
Outpatient management of moderate cellulitis in children using high-dose oral cephalexin.Paediatr Child Health. 2022 May 3;27(4):213-219. doi: 10.1093/pch/pxac031. eCollection 2022 Jul. Paediatr Child Health. 2022. PMID: 35859686 Free PMC article.
-
New Developments in Bacterial, Viral, and Fungal Cutaneous Infections.Curr Dermatol Rep. 2020;9(2):152-165. doi: 10.1007/s13671-020-00295-1. Epub 2020 Mar 5. Curr Dermatol Rep. 2020. PMID: 32435525 Free PMC article. Review.
-
Clinical Impact of Staphylococcus aureus Skin and Soft Tissue Infections.Antibiotics (Basel). 2023 Mar 11;12(3):557. doi: 10.3390/antibiotics12030557. Antibiotics (Basel). 2023. PMID: 36978425 Free PMC article. Review.
References
-
- Hersh AL, Chambers HF, Maselli JH, Gonzales R. National trends in ambulatory visits and antibiotic prescribing for skin and soft-tissue infections. Arch Intern Med. 2008;168(14):1585-1591. - PubMed
-
- Pallin DJ, Egan DJ, Pelletier AJ, Espinola JA, Hooper DC, Camargo CA Jr. Increased US emergency department visits for skin and soft tissue infections, and changes in antibiotic choices, during the emergence of community-associated methicillin-resistant Staphylococcus aureus. Ann Emerg Med. 2008;51(3):291-298. - PubMed
-
- Gunderson CG, Martinello RA. A systematic review of bacteremias in cellulitis and erysipelas. J Infect. 2012;64(2):148-155. - PubMed
-
- Jeng A, Beheshti M, Li J, Nathan R. The role of beta-hemolytic streptococci in causing diffuse, nonculturable cellulitis: a prospective investigation. Medicine (Baltimore). 2010;89(4):217-226. - PubMed
-
- Chira S, Miller LG. Staphylococcus aureus is the most common identified cause of cellulitis: a systematic review. Epidemiol Infect. 2010;138(3):313-317. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
