

Coasting (withholding gonadotrophins) for preventing ovarian hyperstimulation syndrome
- PMID: 28535578
- PMCID: PMC6481358
- DOI: 10.1002/14651858.CD002811.pub4
Coasting (withholding gonadotrophins) for preventing ovarian hyperstimulation syndrome
Abstract
Background: Ovarian hyperstimulation syndrome (OHSS) is an iatrogenic and potentially life threatening condition resulting from excessive ovarian stimulation. Reported incidence of moderate to severe OHSS ranges from 0.6% to 5% of in vitro fertilization (IVF) cycles. The factors contributing to OHSS have not been completely explained. The release of vasoactive substances secreted by the ovaries under human chorionic gonadotrophin (hCG) stimulation may play a key role in triggering this syndrome. This condition is characterised by a massive shift of fluid from the intravascular compartment to the third space, resulting in profound intravascular depletion and haemoconcentration.
Objectives: To assess the effect of withholding gonadotrophins (coasting) on the prevention of ovarian hyperstimulation syndrome in assisted reproduction cycles.
Search methods: For the update of this review, we searched the Cochrane Gynaecology and Fertility Group Trials Register, CENTRAL, MEDLINE (PubMed), CINHAL, PsycINFO, Embase, Google, and clinicaltrials.gov to 6 July 2016.
Selection criteria: We included only randomized controlled trials (RCTs) in which coasting was used to prevent OHSS.
Data collection and analysis: Two review authors independently selected trials and extracted data. They resolved disagreements by discussion. They contacted study authors to request additional information or missing data. The intervention comparisons were coasting versus no coasting, coasting versus early unilateral follicular aspiration (EUFA), coasting versus gonadotrophin releasing hormone antagonist (antagonist), coasting versus follicle stimulating hormone administration at the time of hCG trigger (FSH co-trigger), and coasting versus cabergoline. We performed statistical analysis in accordance with Cochrane guidelines. Our primary outcomes were moderate or severe OHSS and live birth.
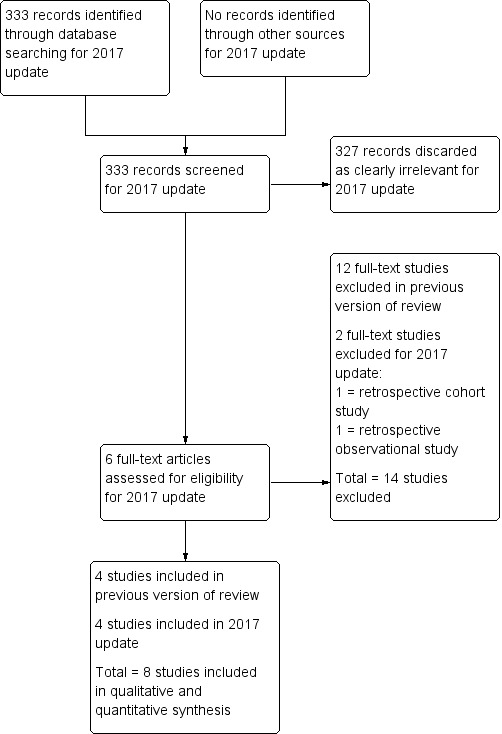
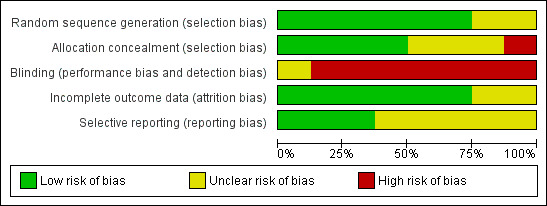
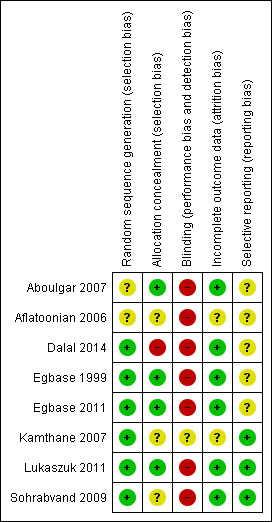
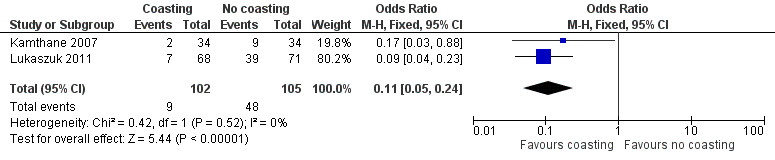
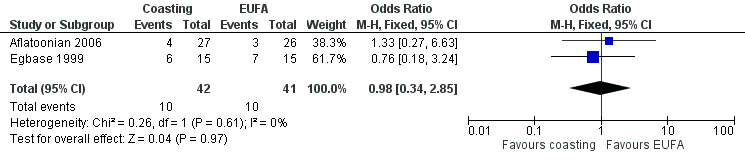
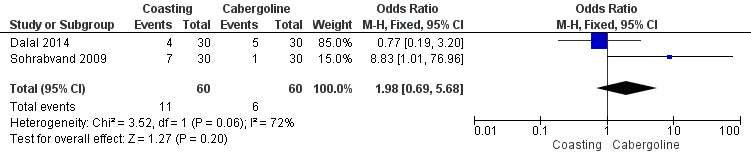
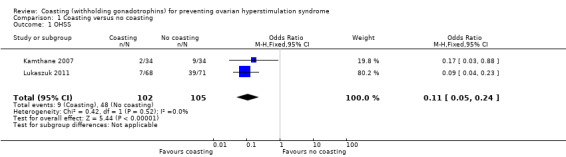
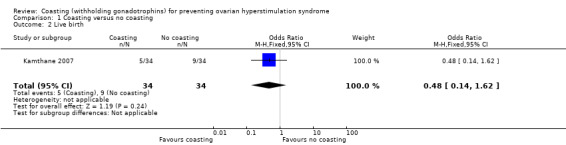
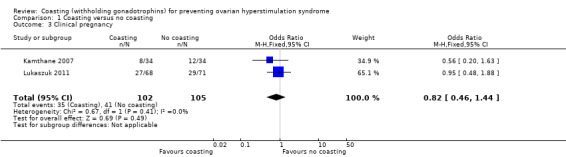
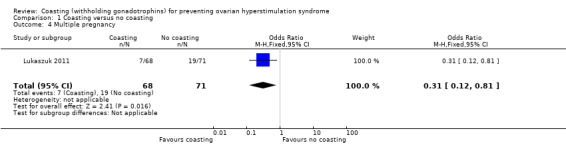
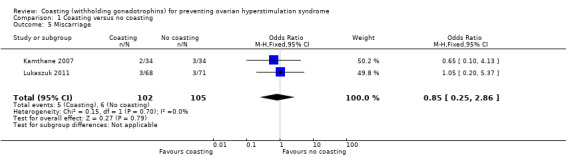
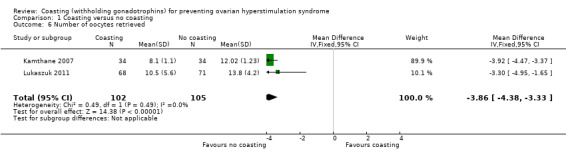
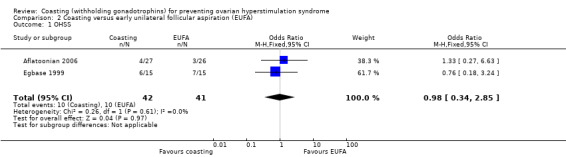
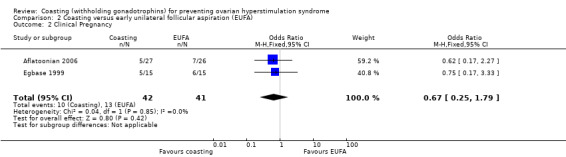
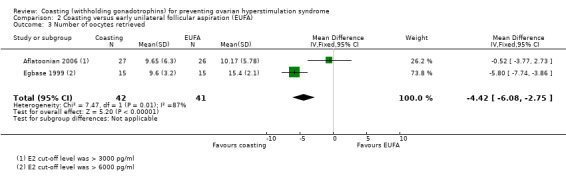
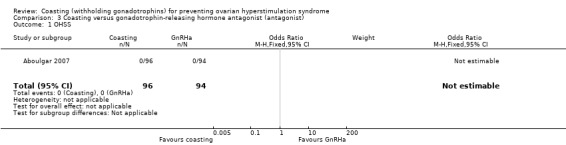
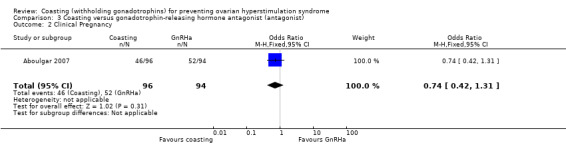
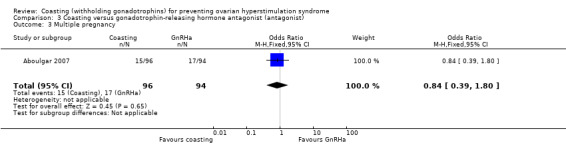
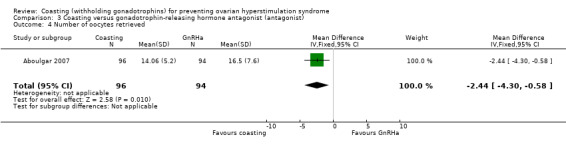
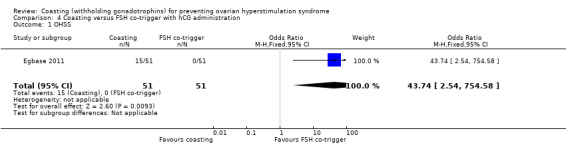
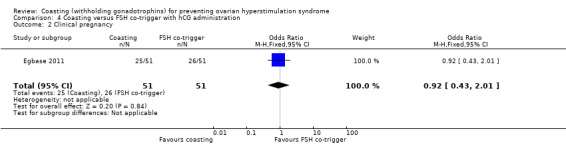
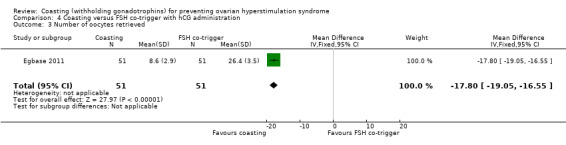
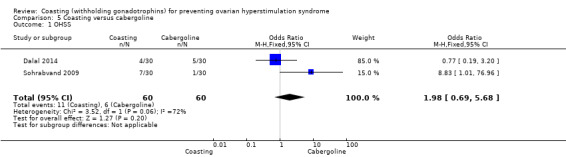
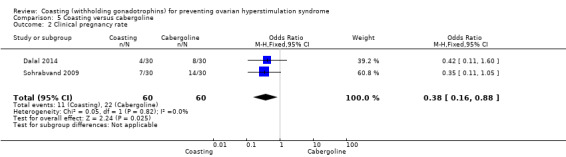
Main results: We included eight RCTs (702 women at high risk of developing OHSS). The quality of evidence was low or very low. The main limitations were failure to report live birth, risk of bias due to lack of information about study methods, and imprecision due to low event rates and lack of data. Four of the studies were published only as abstracts, and provided limited data. Coasting versus no coastingRates of OHSS were lower in the coasting group (OR 0.11, 95% CI 0.05 to 0.24; I² = 0%, two RCTs; 207 women; low-quality evidence), suggesting that if 45% of women developed moderate or severe OHSS without coasting, between 4% and 17% of women would develop it with coasting. There were too few data to determine whether there was a difference between the groups in rates of live birth (OR 0.48, 95% CI 0.14 to 1.62; one RCT; 68 women; very low-quality evidence), clinical pregnancy (OR 0.82, 95% CI 0.46 to 1.44; I² = 0%; two RCTs; 207 women; low-quality evidence), multiple pregnancy (OR 0.31, 95% CI 0.12 to 0.81; one RCT; 139 women; low-quality evidence), or miscarriage (OR 0.85, 95% CI 0.25 to 2.86; I² = 0%; two RCTs; 207 women; very low-quality evidence). Coasting versus EUFAThere were too few data to determine whether there was a difference between the groups in rates of OHSS (OR 0.98, 95% CI 0.34 to 2.85; I² = 0%; 2 RCTs; 83 women; very low-quality evidence), or clinical pregnancy (OR 0.67, 95% CI 0.25 to 1.79; I² = 0%; 2 RCTs; 83 women; very low-quality evidence); no studies reported live birth, multiple pregnancy, or miscarriage. Coasting versus antagonistOne RCT (190 women) reported this comparison, and no events of OHSS occurred in either arm. There were too few data to determine whether there was a difference between the groups in clinical pregnancy rates (OR 0.74, 95% CI 0.42 to 1.31; one RCT; 190 women; low-quality evidence), or multiple pregnancy rates (OR 1.00, 95% CI 0.43 to 2.32; one RCT; 98 women; very low-quality evidence); the study did not report live birth or miscarriage. Coasting versus FSH co-triggerRates of OHSS were higher in the coasting group (OR 43.74, 95% CI 2.54 to 754.58; one RCT; 102 women; very low-quality evidence), with 15 events in the coasting arm and none in the FSH co-trigger arm. There were too few data to determine whether there was a difference between the groups in clinical pregnancy rates (OR 0.92, 95% CI 0.43 to 2.10; one RCT; 102 women; low-quality evidence). This study did not report data suitable for analysis on live birth, multiple pregnancy, or miscarriage, but stated that there was no significant difference between the groups. Coasting versus cabergolineThere were too few data to determine whether there was a difference between the groups in rates of OHSS (OR 1.98, 95% CI 0.09 to 5.68; P = 0.20; I² = 72%; two RCTs; 120 women; very low-quality evidence), with 11 events in the coasting arm and six in the cabergoline arm. The evidence suggested that coasting was associated with lower rates of clinical pregnancy (OR 0.38, 95% CI 0.16 to 0.88; P = 0.02; I² =0%; two RCTs; 120 women; very low-quality evidence), but there were only 33 events altogether. These studies did not report data suitable for analysis on live birth, multiple pregnancy, or miscarriage.
Authors' conclusions: There was low-quality evidence to suggest that coasting reduced rates of moderate or severe OHSS more than no coasting. There was no evidence to suggest that coasting was more beneficial than other interventions, except that there was very low-quality evidence from a single small study to suggest that using FSH co-trigger at the time of HCG administration may be better at reducing the risk of OHSS than coasting. There were too few data to determine clearly whether there was a difference between the groups for any other outcomes.
Conflict of interest statement
ADA, NNA and RH have no conflicts of interest to declare
Figures
Update of
-
Coasting (withholding gonadotrophins) for preventing ovarian hyperstimulation syndrome.Cochrane Database Syst Rev. 2011 Jun 15;(6):CD002811. doi: 10.1002/14651858.CD002811.pub3. Cochrane Database Syst Rev. 2011. Update in: Cochrane Database Syst Rev. 2017 May 23;5:CD002811. doi: 10.1002/14651858.CD002811.pub4. PMID: 21678336 Updated.
References
References to studies included in this review
Aboulgar 2007 {published data only}
-
- Aboulghar M, Mansour R, Amin Y, Al‐Inany H, Aboulghar M, Serour G. A prospective randomized study comparing coasting with GnRH antagonist administration in patients at risk for severe OHSS. Reproductive Biomedicine Online 2007;15(3):271‐9. - PubMed
Aflatoonian 2006 {published data only}
-
- Aflatoonian A, Mahani I, Tabibnejad N, Aflatoonian B, Aflatoonian R. Comparison of coasting with aspiration half of follicles before hCG injection for prevention of OHSS in ART cycles. Human Reproduction 2006;21(Suppl 1):i37.
Dalal 2014 {published and unpublished data}
-
- Dalal R, Mishra A. Comparison of coasting with cabergoline administration for prevention of early severe OHSS in ART cycles. BJOG Eposter 2014:78.
Egbase 1999 {published data only}
-
- Egbase PE, Al Sharhan M, Grudzinskas JG. Early unilateral follicular aspiration compared with coasting for the prevention of severe ovarian hyperstimulation syndrome: a prospective randomized study. Human Reproduction 1999;14(6):1421‐5. - PubMed
Egbase 2011 {published data only}
-
- Egbase P, Al Sharhan M, Masangcay M, Egbase E. Follicle stimulating hormone (FSH) administer with trigger dose human chorionic gonadotropin (hCG) completely prevents ovarian hyperstimulation syndrome (OHSS). Randomised controlled trial. Fertility and Sterility 2011;96(3):S20.
Kamthane 2007 {published data only}
-
- Kamthane V, Goswami S, Ghosh S, Chattopadhay R, Chakravarty B. Does coasting prevent OHSS without compromising pregnancy outcome?. Human Reproduction 2004;19 Suppl(6):i121.
Lukaszuk 2011 {published data only}
-
- Lukaszuk K, Liss J, Jakiel G. 'Internal Coasting' for prevention of ovarian hyperstimulation syndrome (OHSS) in IVF/ICSI. Ginekol Pol 2011;82:812‐6. - PubMed
Sohrabvand 2009 {published data only}
-
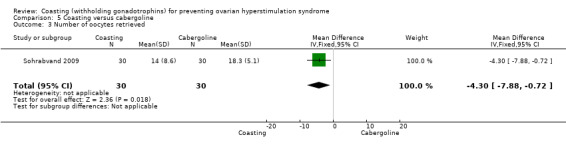
- Sohrabvand F, Ansaripour MD, Bagheri M, Shariat M, Jafarabadi M. Cabergoline versus coasting in the prevention of ovarian hyperstimulation syndrome and assisted reproductive outcome in high risk patients. International Journal of Fertility and Sterility 2009;3(1):35‐40.
References to studies excluded from this review
Aboulghar 1998 {published data only}
-
- Aboulghar MA, Mansour RT, Serour GI, Sattar M, Ranzy AM, Amin Y. Successful prevention of ovarian hyperstimulation syndrome by reduction of human menopausal gonadotrophin dose following by delayed HCG injection. Human Reproduction 1998;13:243‐4.
Al‐Shawaf 2001 {published data only}
-
- Al‐Shawaf T, Zosmer A, Hussain S, Tozer A, Panay N, Wilson C, et al. Prevention of severe ovarian hyperstimulation syndrome in IVF with or without ICSI and embryo transfer: a modified 'coasting' strategy based on ultrasound identification of high‐risk patients. Human Reproduction 2001;1(16):24‐30. - PubMed
Benadiva 1997 {published data only}
-
- Benadiva CA, Davis O, Kligman I, Moomjy M, Hung‐Ching L, Rosenwaks Z. Withholding gonadotropin administration is an effective alternative for the prevention of ovarian hyperstimulation syndrome. Fertility and Sterility 1997;67(4):724‐7. - PubMed
Dhont 1998 {published data only}
-
- Dhont M, Straeten F, Sutter P. Prevention of severe ovarian hyperstimulation by coasting. Fertility and Sterility 1998;70(9):847‐50. - PubMed
Esinler 2013 {published data only}
-
- Esinler I, Bozdag G. Preventing ovarian hyperstimulation syndrome: cabergoline versus coasting. Archives of Gynecology and Obstetrics 2013;288:1159‐63. - PubMed
Fluker 1999 {published data only}
-
- Fluker MR, Hooper WM, Yuzpe A. Withholding gonadotropins ('coasting') to minimize the risk of ovarian hyperstimulation during superovulation and in vitro fertilization‐embryo transfer cycles. Fertility and Sterility 1999;71(2):294‐301. - PubMed
Herrero 2011 {published data only}
-
- Herrero L, Pareja S, Losada C, Cobo AC, Pellicer A, Garcia‐Velasco. Avoiding the use of human chorionic gonadotrophin combined with oocyte vitrification and GnRH agonist versus coasting: a new strategy to avoid ovarian hyperstimulation syndrome.. Fertility and Sterility 2011;95(3):1137‐40. - PubMed
Lee 1998 {published data only}
-
- Lee C, Tummon I, Martin J, Nisker J, Power S, Tekpetey F. Does withholding gonadotropin administration prevent severe ovarian hyperstimulation syndrome?. Human Reproduction 1998;13(5):1157‐8. - PubMed
Sher 1995 {published data only}
-
- Sher G, Zouves C, Feinman M, Maassarani G. 'Prolonged coasting': an effective method for preventing severe ovarian hyperstimulation syndrome in patients undergoing in vitro fertilization. Human Reproduction 1995;10(12):3107‐9. - PubMed
Tortoriello 1998 {published data only}
-
- Tortoriello DV, McGovern P, Colon JM, Skurnick JH, Lipetz K, Santoro N. 'Coasting' does not adversely affect cycle outcome in a subset of highly responsive in vitro fertilization patients. Fertility and Sterility 1998;69(3):454‐60. - PubMed
Tortoriello 1999 {published data only}
-
- Tortoriello DV. Exogenous gonadotropin withdrawal for the prevention of severe ovarian hyperstimulation syndrome: a critical review. Assisted Reproduction 1999;9(1):17‐22.
Ulug 2002 {published data only}
-
- Ulug U, Bahceci M, Erden HF, Shalev E, Ben‐Shlomo I. The significance of coasting duration during ovarian stimulation for conception in assisted fertilization cycles. Human Reproduction 2002;17(2):310‐3. - PubMed
VanderStraeten 1998 {published data only}
-
- Straeten F, Sutter P, Dhont M. Prevention of threatening ovarian hyperstimulation by coasting. Assisted Reproduction 1998;21(4):200‐4.
Waldenstrom 1999 {published data only}
-
- Waldenstrom U, Kahn J, Marsk L, Nilsson S. High pregnancy rates and successful prevention of severe ovarian hyperstimulation syndrome by 'prolonged coasting' of very hyperstimulated patients: a multicentre study. Human Reproduction 1999;14(2):294‐7. - PubMed
Additional references
Agrawal 1999
-
- Agrawal R, Tan SL, Wild S, Sladkevicius P, Engnrann L, Payne N, et al. Serum vascular endothelium growth factor concentrations in in vitro fertilization cycles predict the risk of ovarian hyperstimulation syndrome. Fertility and Sterility 1999;71:287‐93. - PubMed
ASRM 2016
-
- Practice Committee of the American Society for Reproductive Medicine. Prevention and treatment of moderate and severe ovarian hyperstimulation syndrome: a guideline. Fertility and Sterility 2016;106:1634‐47. - PubMed
Calhaz‐Jorge 2016
-
- Calhaz‐Jorge C, Geyter C, Kupka MS, de Mouzon, Erb K, Mocanu E, et al. Assisted reproductive technology in Europe, 2012: results generated from European registers by ESHRE. Human Reproduction 2016;31(8):1638‐52. - PubMed
Golan 1989
-
- Golan A, Ron‐El R, Herman A, Soffer Y, Wainraub Z, Caspi E. Ovarian hyperstimulation syndrome: an update review. Obstetrical and Gynaecological Survey 1989;44:430‐40. - PubMed
Goldsman 1995
-
- Goldsman MP, Pedram A, Dominiguez CE, Ciuffardi I, Levin E, Asch RH. Increased capillary permeability induced by human follicular fluid: a hypothesis for an ovarian origin of the hyperstimulation syndrome. Fertility and Sterility 1995;63:268‐72. - PubMed
GRADEpro GDT 2014 [Computer program]
-
- GRADE Working Group, McMaster University. GRADEpro GDT. Version accessed prior to November 2016. Hamilton (ON): GRADE Working Group, McMaster University, 2014.
Higgins 2011
-
- Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.handbook.cochrane.org.
Kawwass 2015
-
- Kawwass JF, Kissin DM, Kulkarni AD, Creanga AA, Session DR, Callaghan WM, et al. Safety of assisted reproductive technology in the United States, 2000‐2011. JAMA 2015;313(1):88. - PubMed
Navot 1992
-
- Navot D, Bergh PA, Laufer N. Ovarian hyperstimulation syndrome in novel reproductive technologies: prevention and treatment. Fertility and Sterility 1992;58:249‐61. - PubMed
Rabau 1967
-
- Rabau E, Serr DM, David A, Mashiach S, Lunenfield B. Human menopausal gonadotrophins for anovulation and sterility. American Journal of Obstetrics and Gynaecology 1967;98:92‐8. - PubMed
Rizk 1999
-
- Rizk B, Aboulghar MA. Classification, pathophysiology and management of ovarian hyperstimulation syndrome. In: Brinsden P editor(s). A Textbook of In Vitro Fertilization and Assisted Reproduction. 2nd Edition. London: Parthenon Publishing, 1999:131‐55.
Schenker 1978
-
- Schenker JG, Weinstein D. Ovarian hyperstimulation syndrome: a current survey. Fertility and Sterility 1978;30:255‐68. - PubMed
Sher 1993
-
- Sher G, Salem R, Feinman M, Dodge S, Zouves C, Knutzen V. Eliminating the risk of life‐endangering complications following overstimulation with menotropin fertility agents: a report on women undergoing in vitro fertilization and embryo transfer. Obstetrics and Gynaecology 1993;81(6):1009‐11. - PubMed
Tsirigotis 1994
-
- Tsirigotis M, Craft I. Ovarian hyperstimulation syndrome (OHSS): how much do we really know about it?. European Journal of Obstetrics and Gynecology 1994;55(3):151‐5. - PubMed
References to other published versions of this review
D'Angelo 2000
D'Angelo 2002
D'Angelo 2011
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources