

The spleen in liver cirrhosis: revisiting an old enemy with novel targets
- PMID: 28535799
- PMCID: PMC5442653
- DOI: 10.1186/s12967-017-1214-8
The spleen in liver cirrhosis: revisiting an old enemy with novel targets
Abstract
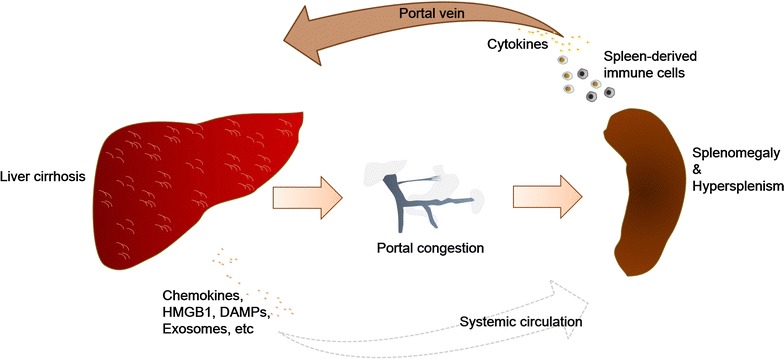
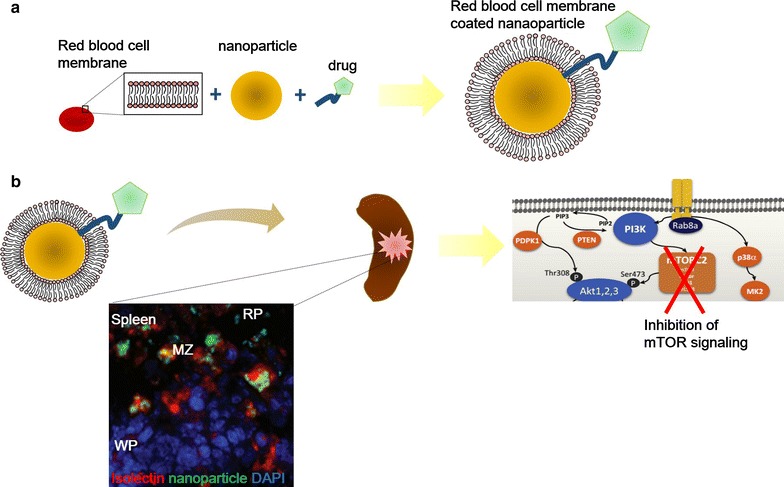
The spleen is a secondary lymphoid organ which can influence the progression of multiple diseases, notably liver cirrhosis. In chronic liver diseases, splenomegaly and hypersplenism can manifest following the development of portal hypertension. These splenic abnormalities correlate with and have been postulated to facilitate the progression of liver fibrosis to cirrhosis, although precise mechanisms remain poorly understood. In this review, we summarize the literature to highlight the mechanistic contributions of splenomegaly and hypersplenism to the development of liver cirrhosis, focusing on three key aspects: hepatic fibrogenesis, hepatic immune microenvironment dysregulation and liver regeneration. We conclude with a discussion of the possible therapeutic strategies for modulating splenic abnormalities, including the novel potential usage of nanomedicine in non-surgically targetting splenic disorders for the treatment of liver cirrhosis.
Keywords: Hepatic fibrogenesis; Hepatic immune microenvironment; Hypersplenism; Liver cirrhosis; Liver regeneration; Nanomedicine; Splenomegaly.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
