

Health-Related Quality of Life in Adult Patients with Common Variable Immunodeficiency Disorders and Impact of Treatment
- PMID: 28536745
- PMCID: PMC5489588
- DOI: 10.1007/s10875-017-0404-8
Health-Related Quality of Life in Adult Patients with Common Variable Immunodeficiency Disorders and Impact of Treatment
Abstract
Purpose: Common variable immunodeficiency disorder (CVID) is a primary immunodeficiency disease (PIDD) often associated with severe and chronic infections. Patients commonly receive immunoglobulin (Ig) treatment to reduce the cycle of recurrent infection and improve physical functioning. However, how Ig treatment in CVID affects quality of life (QOL) has not been thoroughly evaluated. The purpose of a recent Immune Deficiency Foundation (IDF) mail survey was to assess the factors that are associated with QOL in patients with CVID receiving Ig treatment.
Methods: A 75-question survey developed by the IDF and a 12-item Short Form Health Survey (SF-12) to assess QOL were mailed to adults with CVID. Mean SF-12 scores were compared between patients with CVID and the general US adult population normative sample.
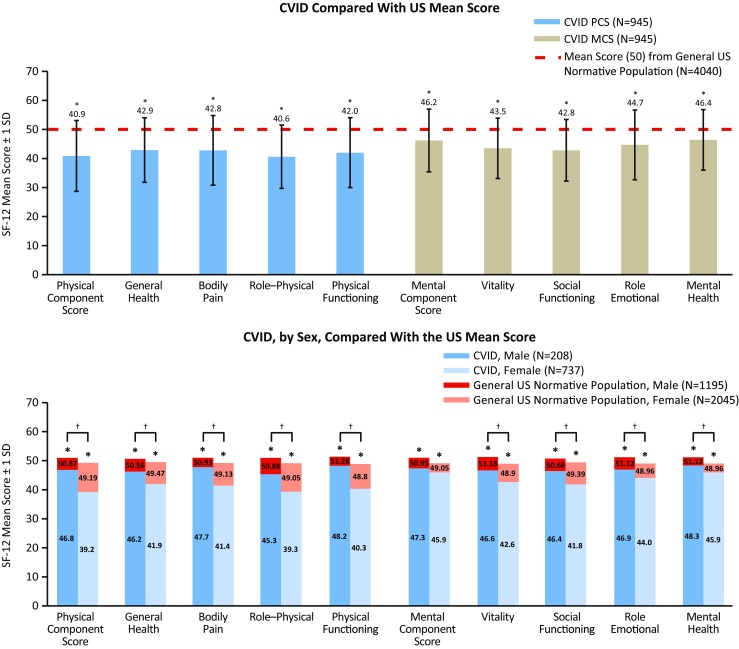
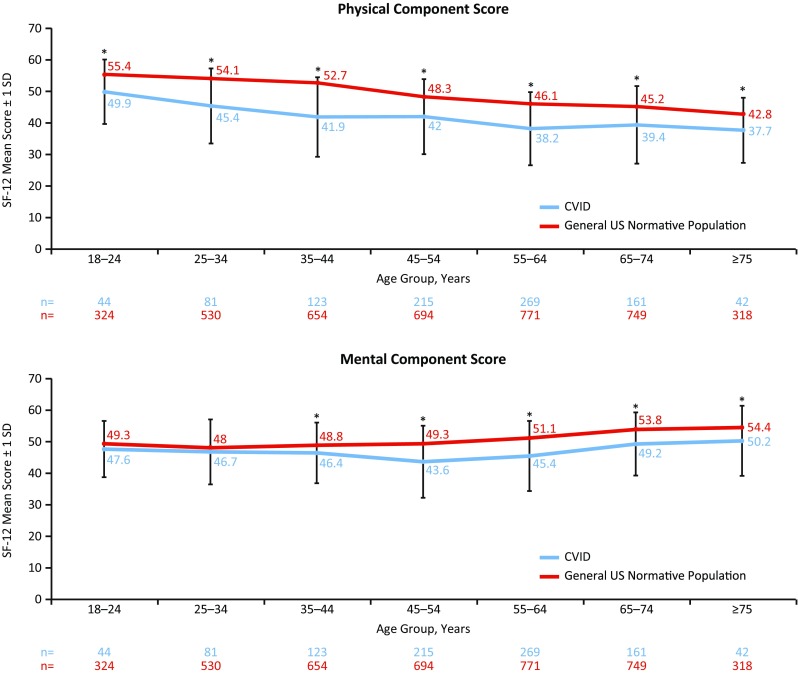
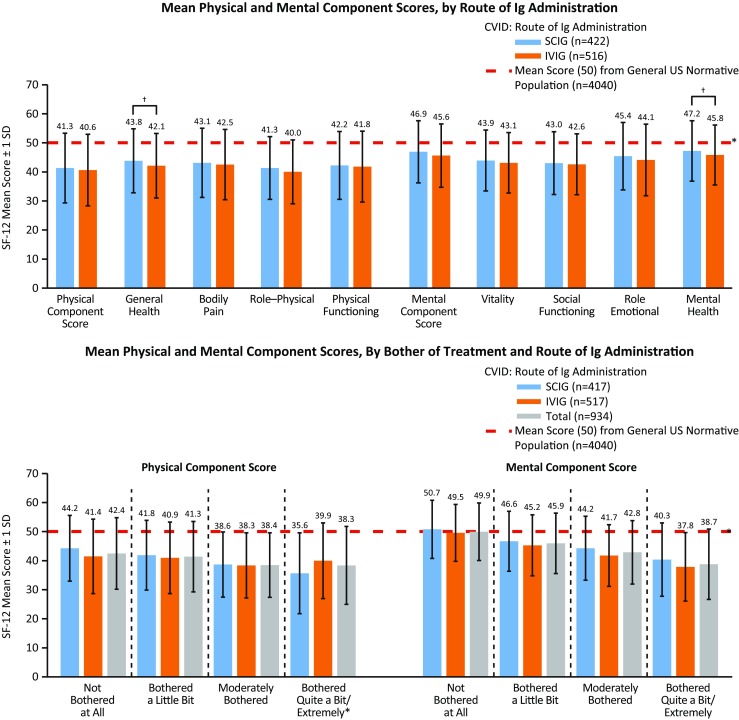
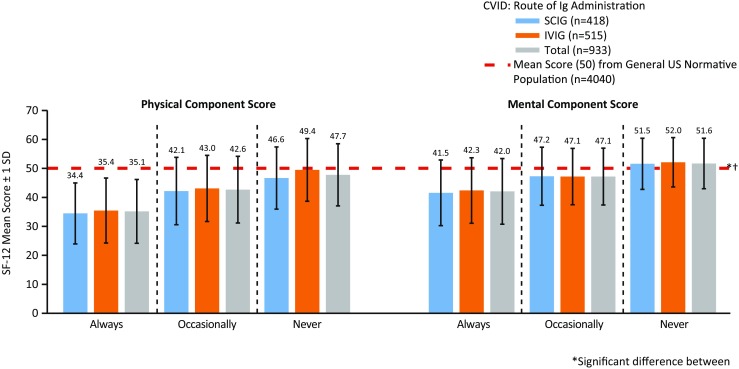
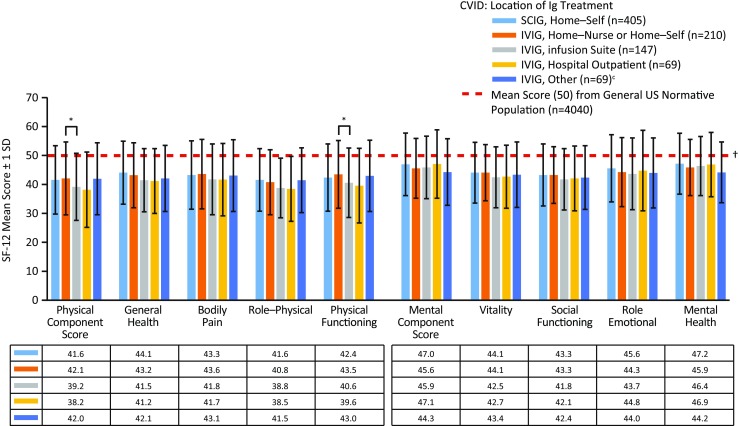
Results: Overall, 945 patients with CVID completed the surveys. More than half of the patients (54.9%) received intravenous Ig and 44.9% received subcutaneous Ig treatment. Patients with CVID had significantly lower SF-12 scores compared with the general US population regardless of sex or age (p < 0.05). Route of IgG replacement did not dramatically improve QOL. SF-12 scores were highest in patients with CVID who have well-controlled PIDD, lacked physical impairments, were not bothered by treatment, and received Ig infusions at home.
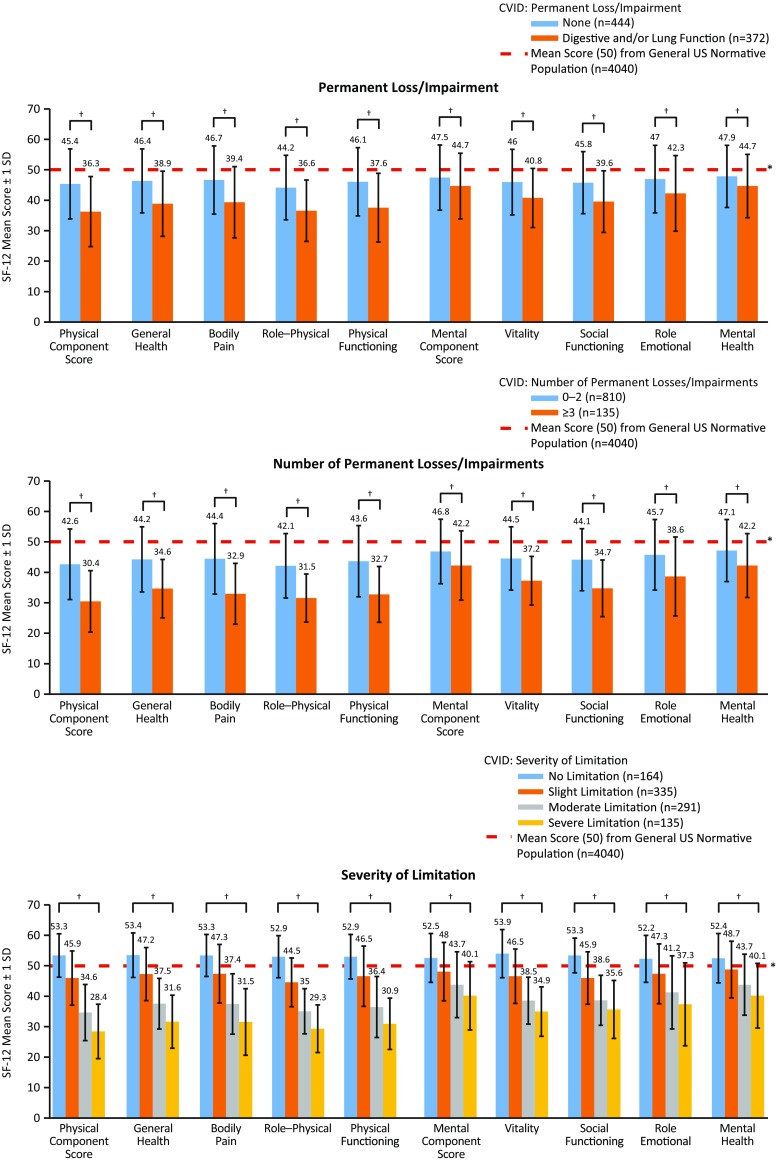
Conclusion: These data provide insight into what factors are most associated with physical and mental health, which can serve to improve QOL in patients in this population. Improvements in QOL can result from early detection of disease, limiting digestive system disease, attention to fatigue, and implementation of an individual treatment plan for the patient.
Keywords: Primary immunodeficiency diseases; common variable immunodeficiency; mental health; physical health; quality of life; reported health.
Conflict of interest statement
Conflict of Interest
NLR and JH have no conflicts to declare. MB, CK, and CS are employees of the Immune Deficiency Foundation (IDF)—IDF has received unrestricted educational grants from Baxalta Inc. for the support of this and other surveys. FOS received grants from Baxalta. JSO received research or educational grants from CSL Behring and Baxalta; received personal consulting fees from CSL Behring, Baxalta, ASD, Walgreens, Grifols, and ADMA; and serves on the medical advisory council to the IDF.
Ethical Statement
Prior to the implementation of this project, the IDF had not, as matter of routine, published findings from IDF surveys in peer-reviewed journals. As such, a protocol for this survey was not submitted to an IRB for consideration for an exemption from need for IRB oversight.
Figures
References
-
- Immune Deficiency Foundation. Treatment experiences and preferences among patients with primary immunodeficiency diseases: 2007. National Survey of Patients. May 1, 2009a. http://primaryimmune.org/idf-survey-research-center/idf-surveys?aid=1264.... Accessed 28 Jul 2016.
-
- Leiva LE, Bezrodnik L, Oleastro M, Condino-Neto A, Costa-Carvalho BT, Grumach AS, et al. Primary immunodeficiency diseases in Latin America: proceedings of the Second Latin American Society for Immunodeficiencies (LASID) Advisory Board. Allergol Immunopathol. 2011;39(2):106–110. doi: 10.1016/j.aller.2010.10.007. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
