

Which Foetal-Pelvic Variables Are Useful for Predicting Caesarean Section and Instrumental Assistance?
- PMID: 28538223
- PMCID: PMC5768136
- DOI: 10.1159/000477732
Which Foetal-Pelvic Variables Are Useful for Predicting Caesarean Section and Instrumental Assistance?
Abstract
Objective: To assess the variables useful to predict caesarean delivery (CD) and instrumental assistance, through the analysis of a large number of foetal-pelvic variables, using discriminant analysis.
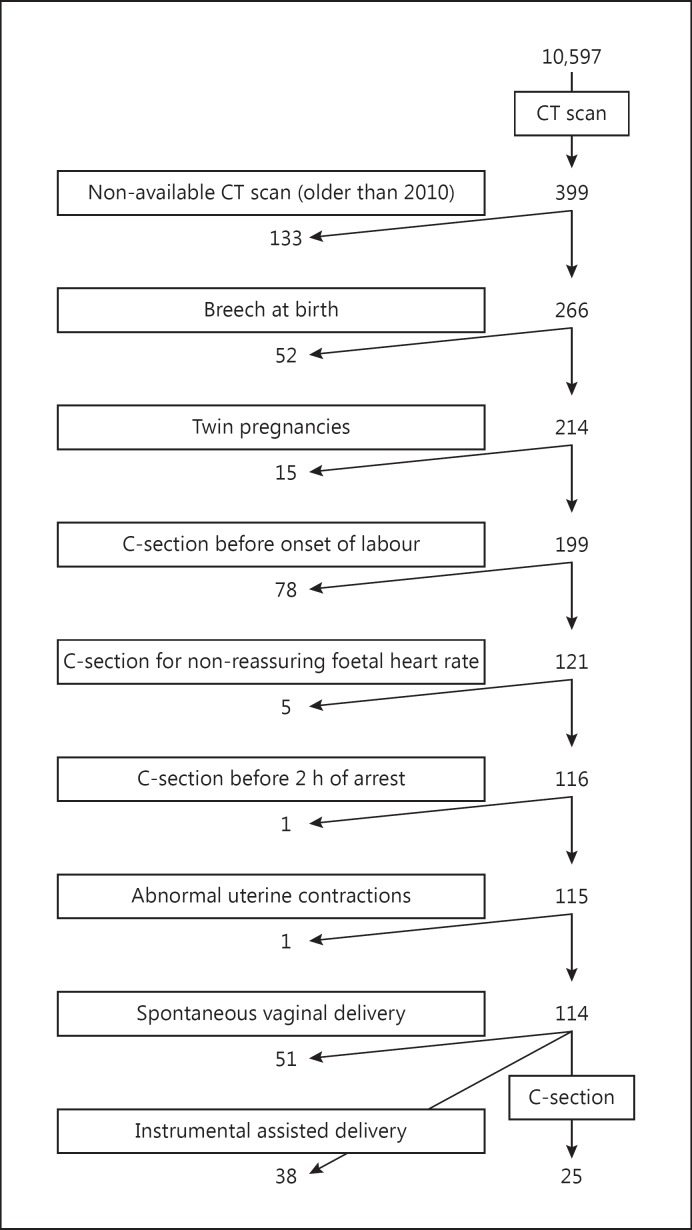
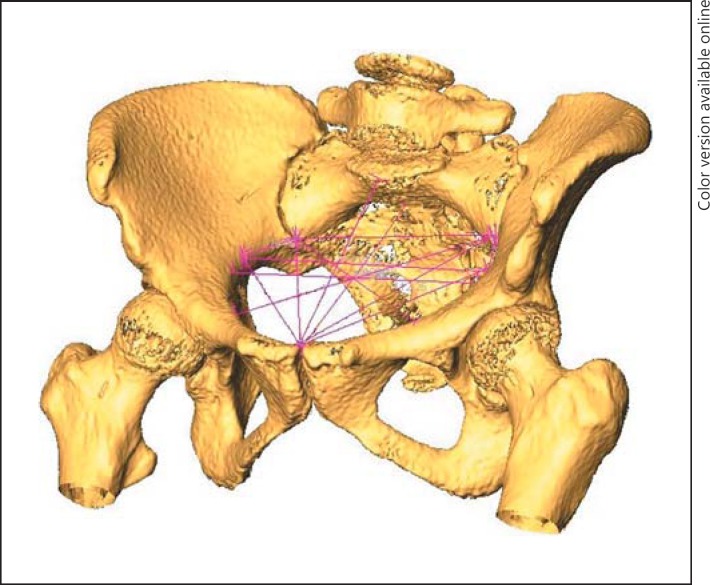
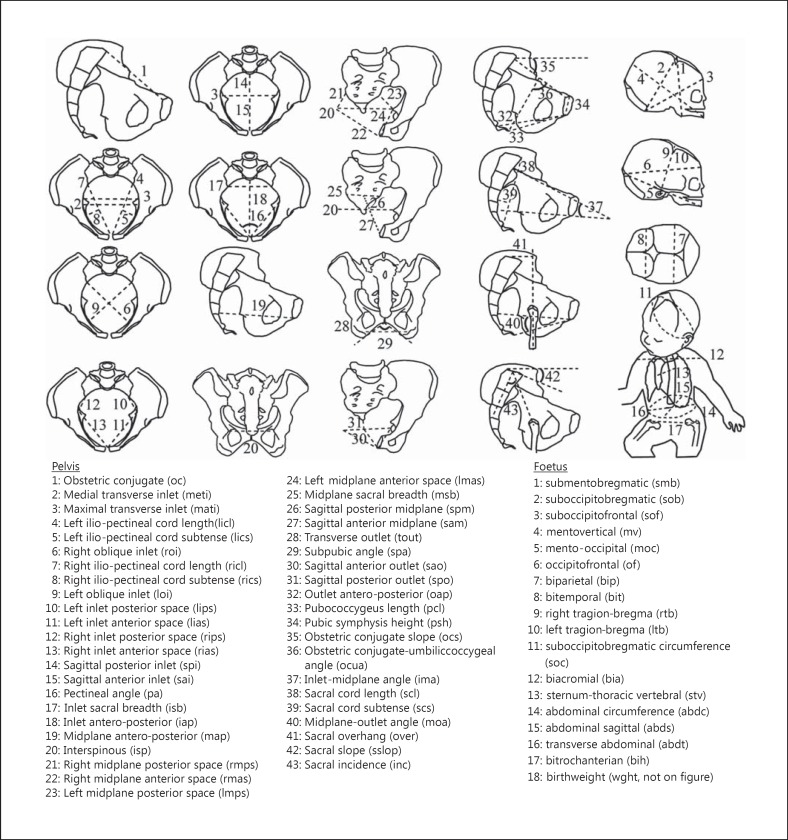
Materials and methods: One hundred and fourteen pregnant women were included in this single-centre prospective study. For each mother-foetus pair, 43 pelvic and 18 foetal variables were measured. Partial least squares-discriminant analysis was performed to identify foetal-pelvic variables that could statistically separate the 3 delivery modality groups: spontaneous vaginal delivery (SVD), CD, and instrument-assisted delivery (IAD).
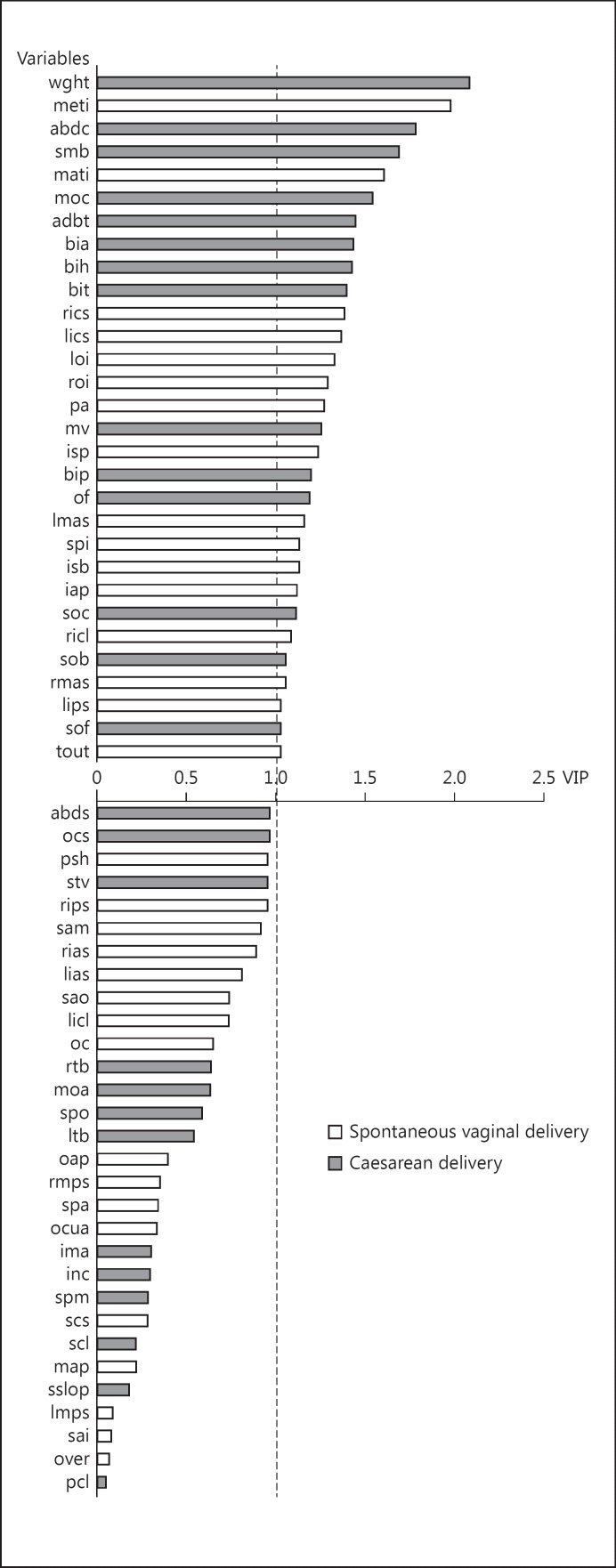
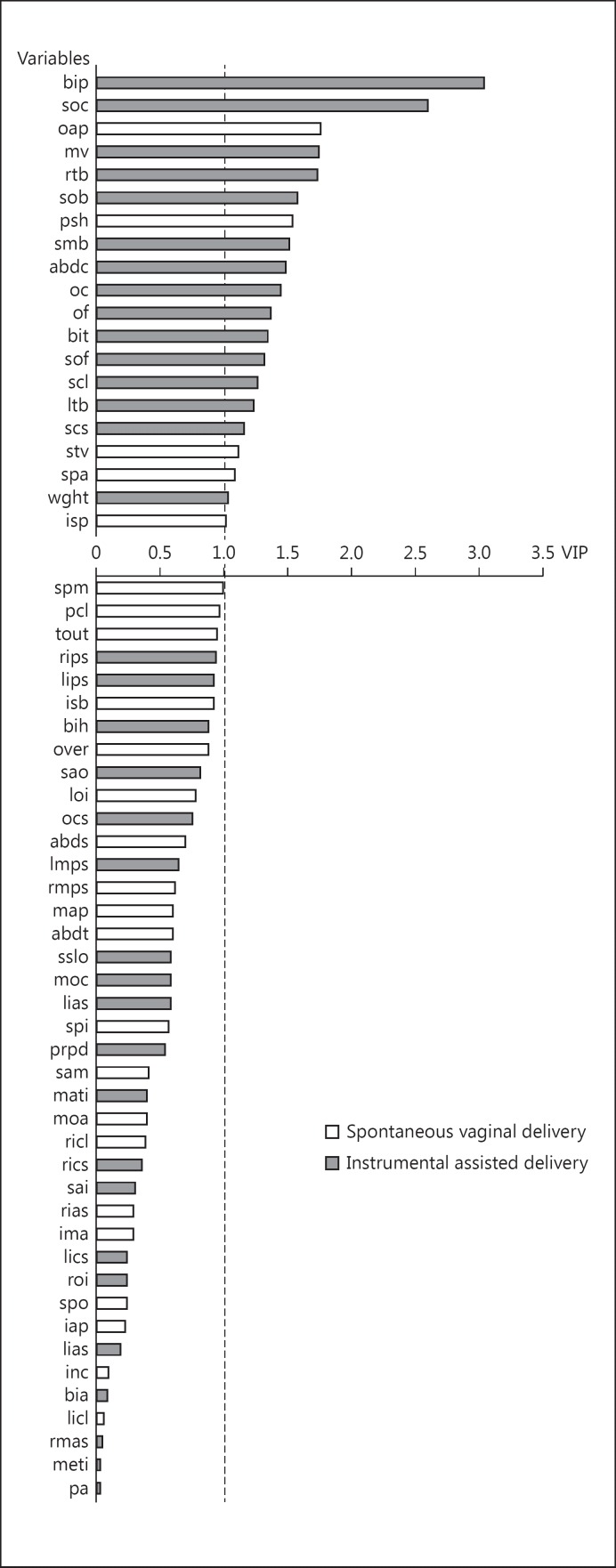
Results: For the SVD versus CD model, voluminous foetuses and women with a narrow pelvic inlet had a greater risk for requiring CD. The most efficient variables for discrimination were the transverse diameter and foetal weight. The antero-posterior inlet and obstetric conjugate were considered in this model, with the former being a useful variable but not the latter. For the SVD versus IAD model, the most important variables were the foetal variables, particularly the bi-parietal diameter. Women with a reduced antero-posterior outlet diameter and a narrow pubic arch were more at risk of requiring an IAD.
Conclusion: The antero-posterior inlet was an efficient variable unlike the obstetric conjugate. The obstetric conjugate diameter should no longer be considered a useful variable in estimating the arrest of labour. Antero-posterior inlet diameter was a sagittal variable that should be taken into account. The comparison of sub-pubic angle and bi-parietal and antero-posterior outlet diameters was useful in identifying a risk of requiring instrumental assistance.
Keywords: Assisted delivery; Caesarean delivery; Foetal-pelvic disproportion; Pelvic scan; Pelvimetry.
© 2017 S. Karger AG, Basel.
Figures
Similar articles
-
Three-dimensional magnetic resonance pelvimetry: A new technique for evaluating the female pelvis in pregnancy.Eur J Radiol. 2018 May;102:208-212. doi: 10.1016/j.ejrad.2018.03.024. Epub 2018 Mar 19. Eur J Radiol. 2018. PMID: 29685537
-
Is X-ray pelvimetry useful in a trial of labour after caesarean section?Eur J Obstet Gynecol Reprod Biol. 1987 Apr;24(4):277-83. doi: 10.1016/0028-2243(87)90152-3. Eur J Obstet Gynecol Reprod Biol. 1987. PMID: 3582716
-
Vaginal delivery of breech presentation.J Obstet Gynaecol Can. 2009 Jun;31(6):557-566. doi: 10.1016/S1701-2163(16)34221-9. J Obstet Gynaecol Can. 2009. PMID: 19646324 English, French.
-
Evolution of the human pelvis and obstructed labor: new explanations of an old obstetrical dilemma.Am J Obstet Gynecol. 2020 Jan;222(1):3-16. doi: 10.1016/j.ajog.2019.06.043. Epub 2019 Jun 25. Am J Obstet Gynecol. 2020. PMID: 31251927 Free PMC article. Review.
-
[Gentle obstetrical management for very early preterm deliveries].Gynakol Geburtshilfliche Rundsch. 2004 Jan;44(1):10-18. doi: 10.1159/000074312. Gynakol Geburtshilfliche Rundsch. 2004. PMID: 14673223 Review. German.
Cited by
-
Childbirth simulation to assess cephalopelvic disproportion and chances for failed labor in a French population.Sci Rep. 2023 Jan 20;13(1):1110. doi: 10.1038/s41598-023-28459-6. Sci Rep. 2023. PMID: 36670300 Free PMC article.
-
Reconsidering the developmental origins of adult disease paradigm: The 'metabolic coordination of childbirth' hypothesis.Evol Med Public Health. 2024 Jan 18;12(1):50-66. doi: 10.1093/emph/eoae002. eCollection 2024. Evol Med Public Health. 2024. PMID: 38380130 Free PMC article. Review.
-
Accuracy and Reliability of Pelvimetry Measures Obtained by Manual or Automatic Labeling of Three-Dimensional Pelvic Models.J Clin Med. 2024 Jan 25;13(3):689. doi: 10.3390/jcm13030689. J Clin Med. 2024. PMID: 38337383 Free PMC article.
-
Obstetrical Constraints and the Origin of Extended Postnatal Brain Maturation in Hominin Evolution.Biology (Basel). 2024 May 31;13(6):398. doi: 10.3390/biology13060398. Biology (Basel). 2024. PMID: 38927278 Free PMC article.
-
Pelvic inlet area is associated with birth mode.Acta Obstet Gynecol Scand. 2023 Jan;102(1):59-66. doi: 10.1111/aogs.14478. Epub 2022 Nov 1. Acta Obstet Gynecol Scand. 2023. PMID: 36320156 Free PMC article.
References
-
- Lurie S, Raz N, Boaz M, et al. Comparison of maternal outcomes from primary cesarean section during the second compared with first stage of labor by indication for the operation. Eur J Obstet Gynecol Reprod Biol. 2014;182:43–47. - PubMed
-
- Ferguson JE, Newberry YG, DeAngelis GA, et al. The fetal-pelvic index has minimal utility in predicting fetal-pelvic disproportion. Am J Obstet Gynecol. 1998;179:1186–1192. - PubMed
-
- Spörri S, Thoeny HC, Raio L, et al. MR imaging pelvimetry: a useful adjunct in the treatment of women at risk for dystocia? AJR Am J Roentgenol. 2002;179:137–144. - PubMed
-
- Pattinson RC, Farrell EE. Pelvimetry for fetal cephalic presentations at term. Cochrane Database Syst Rev. 1997;2:CD000161. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
