

Characteristics of and risk factors for severe neurological deficit in patients with pyogenic vertebral osteomyelitis: A case-control study
- PMID: 28538361
- PMCID: PMC5457841
- DOI: 10.1097/MD.0000000000006387
Characteristics of and risk factors for severe neurological deficit in patients with pyogenic vertebral osteomyelitis: A case-control study
Abstract
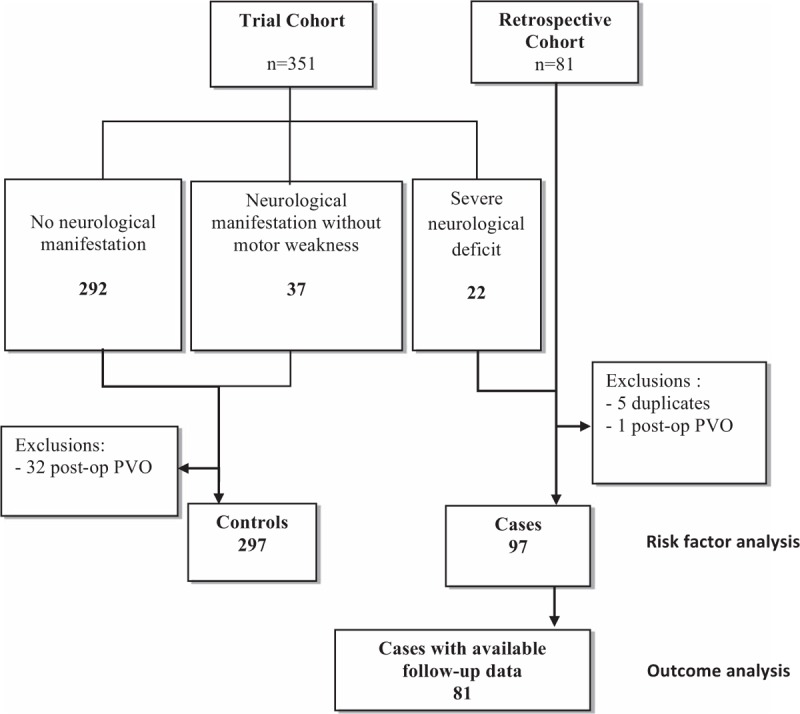
Severe neurological deficit (SND) is a rare but major complication of pyogenic vertebral osteomyelitis (PVO). We aimed to determine the risk factors and the variables associated with clinical improvement for SND during PVO.This case-control study included patients without PVO-associated SND enrolled in a prospective randomized antibiotic duration study, and patients with PVO-associated SND managed in 8 French referral centers. Risk factors for SND were determined by logistic regression.Ninety-seven patients with PVO-associated SND cases, and 297 controls were included. Risk factors for SND were epidural abscess [adjusted odds ratio, aOR 8.9 (3.8-21)], cervical [aOR 8.2 (2.8-24)], and/or thoracic involvement [aOR 14.8 (5.6-39)], Staphylococcus aureus PVO [aOR 2.5 (1.1-5.3)], and C-reactive protein (CRP) >150 mg/L [aOR 4.1 (1.9-9)]. Among the 81 patients with PVO-associated SND who were evaluated at 3 months, 62% had a favorable outcome, defined as a modified Rankin score ≤ 3. No factor was found significantly associated with good outcome, whereas high Charlson index [adjusted Hazard Ratio (aHR) 0.3 (0.1-0.9)], low American Spinal Injury Association (ASIA) impairment scale at diagnosis [aHR 0.4 (0.2-0.9)], and thoracic spinal cord compression [aHR 0.2 (0.08-0.5)] were associated with poor outcome. Duration of antibiotic treatment was not associated with functional outcome.SND is more common in cervical, thoracic, and S. aureus PVO, in the presence of epidural abscess, and when CRP >150 mg/L. Although neurological deterioration occurs in 30% of patients in early follow-up, the functional outcome is quite favorable in most cases after 3 months. The precise impact of optimal surgery and/or corticosteroids therapy must be specified by further studies.
Figures


References
-
- Gouliouris T, Aliyu SH, Brown NM. Spondylodiscitis: update on diagnosis and management. J Antimicrob Chemother 2010;65(Suppl 3):iii11–24. - PubMed
-
- Jensen AG, Espersen F, Skinhøj P, et al. Increasing frequency of vertebral osteomyelitis following Staphylococcus aureus bacteraemia in Denmark 1980-1990. J Infect 1997;34:113–8. - PubMed
-
- Kehrer M, Pedersen C, Jensen TG, et al. Increasing incidence of pyogenic spondylodiscitis: a 14-year population-based study. J Infect 2014;68:313–20. - PubMed
-
- Eismont FJ, Bohlman HH, Soni PL, et al. Pyogenic and fungal vertebral osteomyelitis with paralysis. J Bone Joint Surg Am 1983;65:19–29. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
