

Pregabalin can decrease acute pain and morphine consumption in laparoscopic cholecystectomy patients: A meta-analysis of randomized controlled trials
- PMID: 28538404
- PMCID: PMC5457884
- DOI: 10.1097/MD.0000000000006982
Pregabalin can decrease acute pain and morphine consumption in laparoscopic cholecystectomy patients: A meta-analysis of randomized controlled trials
Abstract
Background: Pregabalin has been used as an adjunct for the management of acute pain in laparoscopic cholecystectomy. This meta-analysis aimed to illustrate the efficacy and safety of pregabalin for pain management following laparoscopic cholecystectomy.
Methods: In March 2017, a systematic computer-based search was conducted in PubMed, EMBASE, Web of Science, Cochrane Database of Systematic Reviews, and Google databases. Data on patients prepared for laparoscopic cholecystectomy in studies that compared pregabalin versus placebo were retrieved. The primary endpoints were the visual analog scale (VAS) score with rest or mobilization at 6, 12, and 24 hours and total morphine consumption. The secondary outcomes were the morphine-related complications (i.e., nausea, vomiting, dizziness, somnolence, headache, pruritus, urine retention, respiratory depression, and blurred vision). Continuous outcomes were expressed as the weighted mean difference (WMD) with a corresponding 95% confidence interval (CI), and discontinuous outcomes were expressed as a risk ratio (RR) with a corresponding 95% CI.
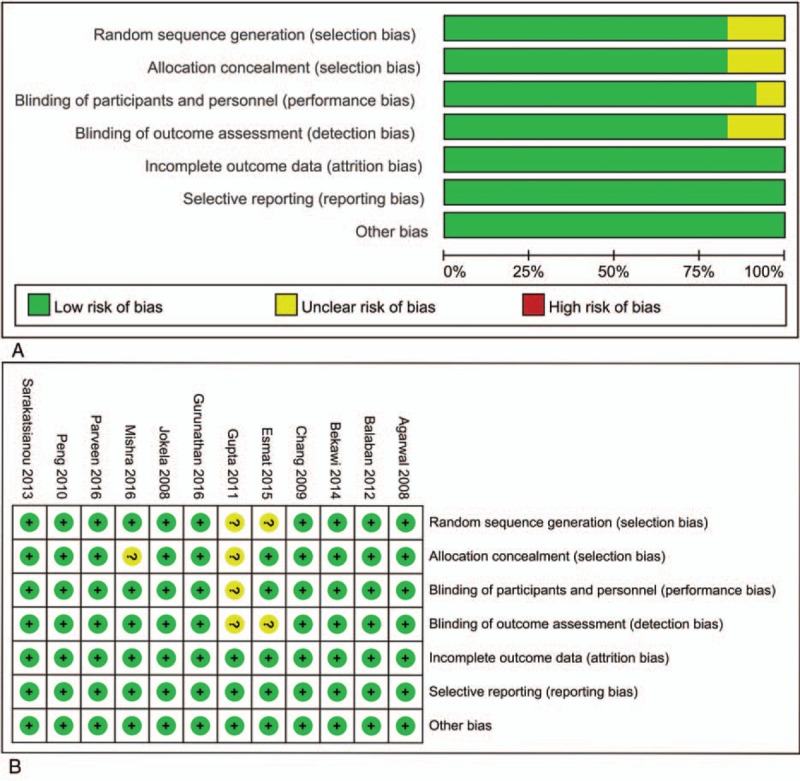
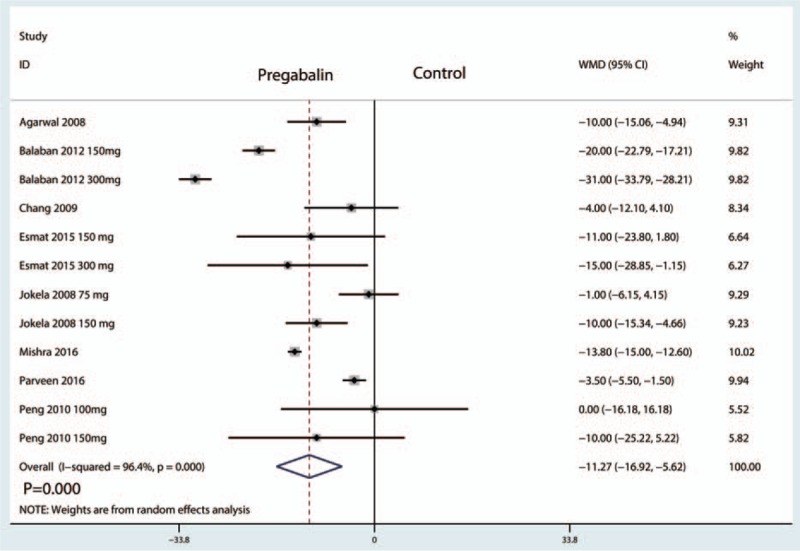
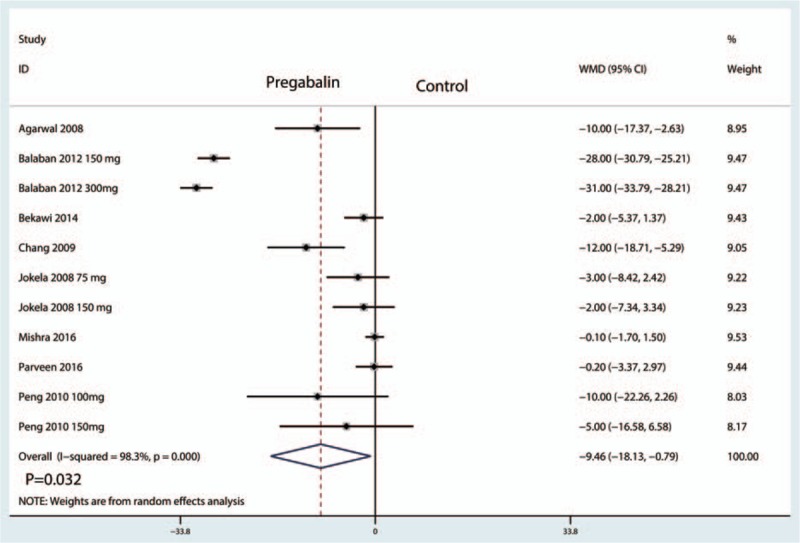
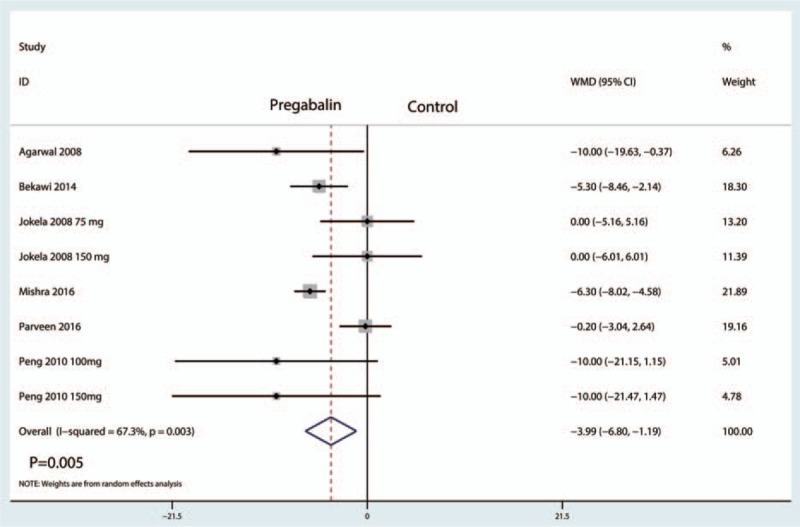
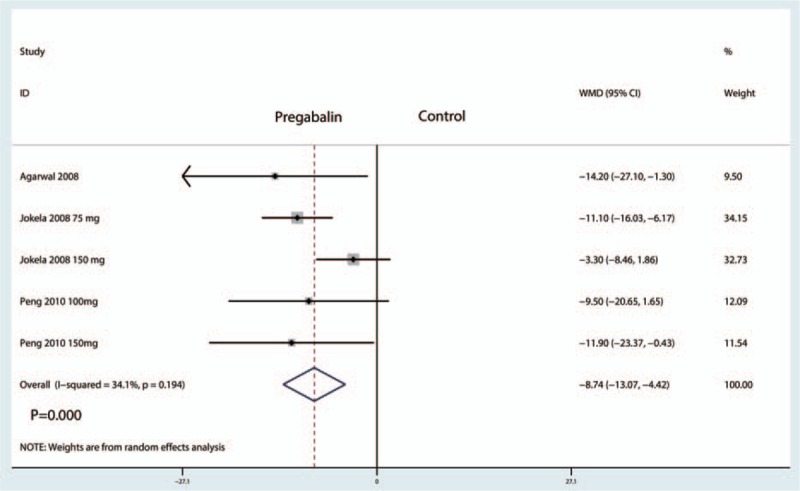
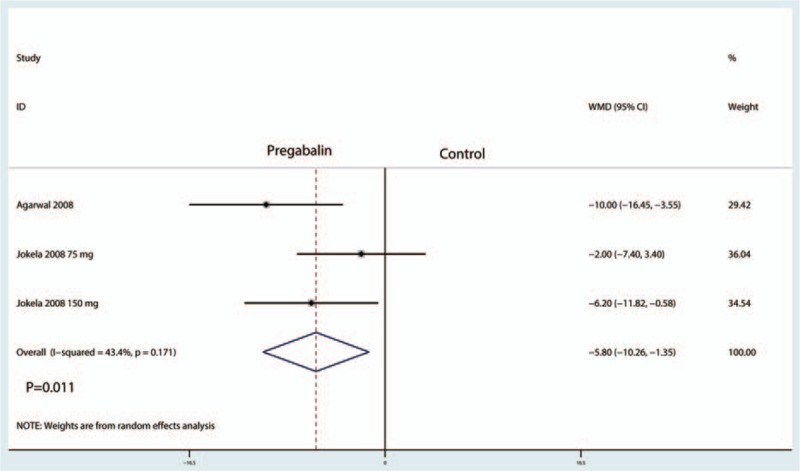
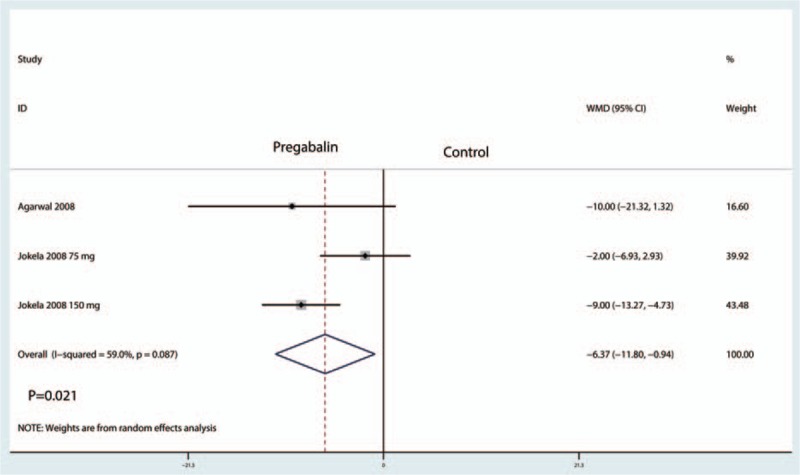
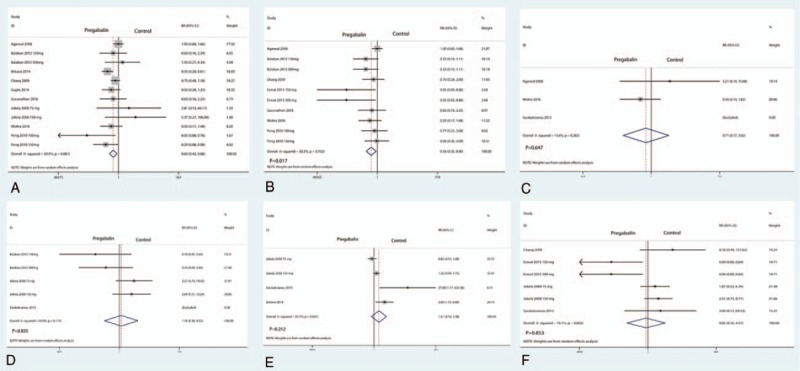
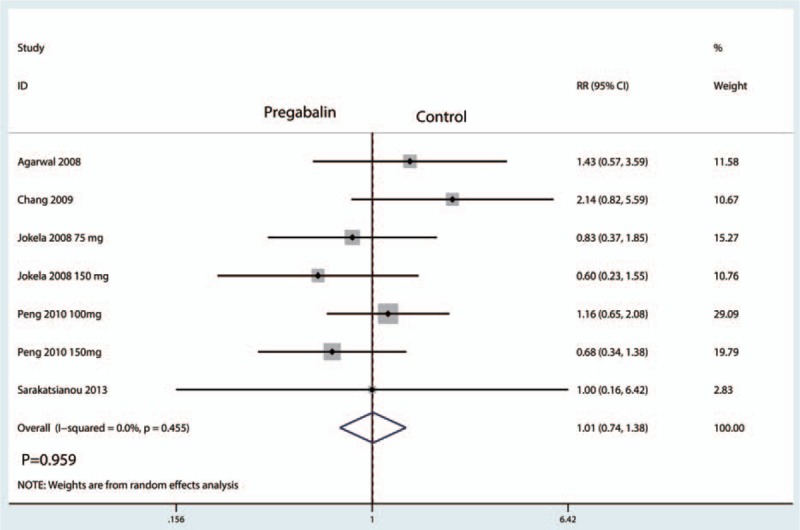
Results: Twelve clinical studies with 938 patients (gabapentin group = 536, control group = 402) were ultimately included in the meta-analysis. Pregabalin was associated with reduced pain scores with rest at 6, 12, and 24 hours, which corresponded to a reduction of 11.27 points at 6 hours, 9.46 points at 12 hours, and 3.99 points at 24 hours on a 100-point VAS. Moreover, pregabalin was associated with reduced pain scores with mobilization at 6, 12, and 24 hours, which corresponded to a reduction of 8.74 points, 5.80 points and 6.37 points at 6, 12, and 24 hours, respectively, on a 110-point VAS. Furthermore, pregabalin reduced the occurrence of nausea and vomiting. There were no significant differences in the occurrence of respiratory depression, pruritus, dizziness, blurred vision, and headache.
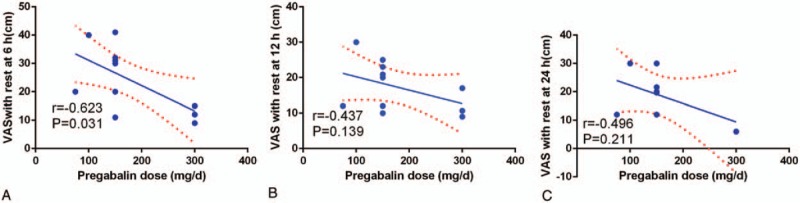
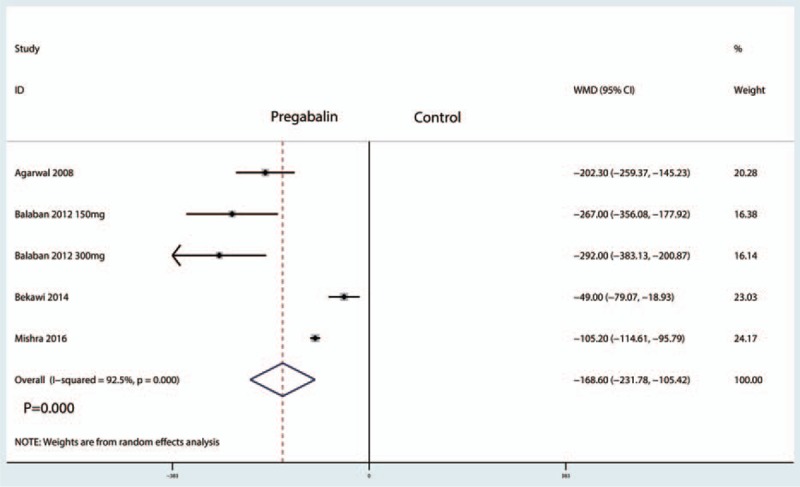
Conclusions: Pregabalin was efficacious in the reduction of postoperative pain, total morphine consumption, and morphine-related complications following laparoscopic cholecystectomy. In addition, a high dose of pregabalin was more effective than a low dose. The dose of pregabalin differed across the studies, and the heterogeneity was large. More studies are needed to verify the optimal dose of pregabalin in laparoscopic cholecystectomy patients.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures

Similar articles
-
Gabapentin can decrease acute pain and morphine consumption in spinal surgery patients: A meta-analysis of randomized controlled trials.Medicine (Baltimore). 2017 Apr;96(15):e6463. doi: 10.1097/MD.0000000000006463. Medicine (Baltimore). 2017. PMID: 28403075 Free PMC article.
-
A meta-analysis of the preoperative use of gabapentinoids for the treatment of acute postoperative pain following spinal surgery.Medicine (Baltimore). 2017 Sep;96(37):e8031. doi: 10.1097/MD.0000000000008031. Medicine (Baltimore). 2017. PMID: 28906391 Free PMC article.
-
Preoperative use of pregabalin for acute pain in spine surgery: A meta-analysis of randomized controlled trials.Medicine (Baltimore). 2017 Mar;96(11):e6129. doi: 10.1097/MD.0000000000006129. Medicine (Baltimore). 2017. PMID: 28296725 Free PMC article.
-
The efficacy of gabapentin in reducing pain intensity and postoperative nausea and vomiting following laparoscopic cholecystectomy: A meta-analysis.Medicine (Baltimore). 2017 Sep;96(37):e8007. doi: 10.1097/MD.0000000000008007. Medicine (Baltimore). 2017. PMID: 28906382 Free PMC article.
-
Clinical study evaluating pregabalin efficacy and tolerability for pain management in patients undergoing laparoscopic cholecystectomy.Clin J Pain. 2014 Nov;30(11):944-52. doi: 10.1097/AJP.0000000000000060. Clin J Pain. 2014. PMID: 24662499 Clinical Trial.
Cited by
-
Quadratus Lumborum Block III for Postoperative Pain After Percutaneous Nephrolithotomy.Turk J Anaesthesiol Reanim. 2018 Aug;46(4):272-275. doi: 10.5152/TJAR.2018.92331. Epub 2018 Aug 1. Turk J Anaesthesiol Reanim. 2018. PMID: 30140533 Free PMC article.
-
Reduction of Acute Postoperative Pain With Pre-Emptive Pregabalin Following Laparoscopic Cholecystectomy.Cureus. 2022 Aug 8;14(8):e27783. doi: 10.7759/cureus.27783. eCollection 2022 Aug. Cureus. 2022. PMID: 36106290 Free PMC article.
-
Perioperative pain management in COVID-19 patients: Considerations and recommendations by the Saudi Anesthesia Society (SAS) and Saudi Society of Pain Medicine (SSPM).Saudi J Anaesth. 2021 Jan-Mar;15(1):59-69. doi: 10.4103/sja.SJA_765_20. Epub 2021 Jan 5. Saudi J Anaesth. 2021. PMID: 33824647 Free PMC article.
-
The effect of preemptive use of pregabalin on postoperative morphine consumption and analgesia levels after laparoscopic colorectal surgery: a controlled randomized trial.Int J Colorectal Dis. 2020 Feb;35(2):323-331. doi: 10.1007/s00384-019-03471-3. Epub 2019 Dec 20. Int J Colorectal Dis. 2020. PMID: 31863206 Clinical Trial.
-
Perioperative use of gabapentinoids for the management of postoperative acute pain: protocol of a systematic review and meta-analysis.Syst Rev. 2019 Jan 16;8(1):24. doi: 10.1186/s13643-018-0906-3. Syst Rev. 2019. PMID: 30651123 Free PMC article.
References
-
- Wilson RG, Macintyre IM. Symptomatic outcome after laparoscopic cholecystectomy. Br J Surg 1993;80:439–41. - PubMed
-
- Apfelbaum JL, Chen C, Mehta SS, et al. Postoperative pain experience: results from a national survey suggest postoperative pain continues to be undermanaged. Anesth Analg 2003;97:534–40. table of contents. - PubMed
-
- Ravindran D. Chronic postsurgical pain: prevention and management. J Pain Palliat Care Pharmacother 2014;28:51–3. - PubMed
-
- Dong J, Li W, Wang Y. The effect of pregabalin on acute postoperative pain in patients undergoing total knee arthroplasty: a meta-analysis. Int J Surg 2016;34:148–60. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
