

A Multivariate Model for Prediction of Obstructive Coronary Disease in Patients with Acute Chest Pain: Development and Validation
- PMID: 28538760
- PMCID: PMC5421469
- DOI: 10.5935/abc.20170037
A Multivariate Model for Prediction of Obstructive Coronary Disease in Patients with Acute Chest Pain: Development and Validation
Abstract
Background:: Currently, there is no validated multivariate model to predict probability of obstructive coronary disease in patients with acute chest pain.
Objective:: To develop and validate a multivariate model to predict coronary artery disease (CAD) based on variables assessed at admission to the coronary care unit (CCU) due to acute chest pain.
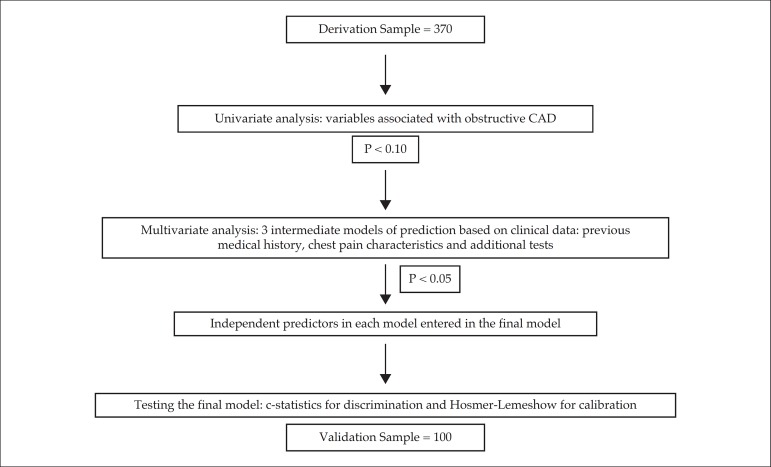
Methods:: A total of 470 patients were studied, 370 utilized as the derivation sample and the subsequent 100 patients as the validation sample. As the reference standard, angiography was required to rule in CAD (stenosis ≥ 70%), while either angiography or a negative noninvasive test could be used to rule it out. As predictors, 13 baseline variables related to medical history, 14 characteristics of chest discomfort, and eight variables from physical examination or laboratory tests were tested.
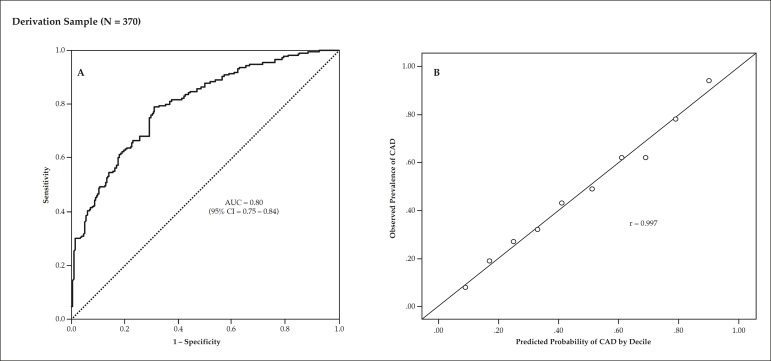
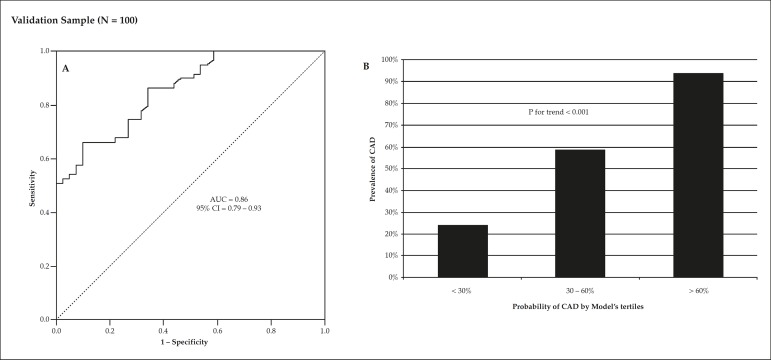
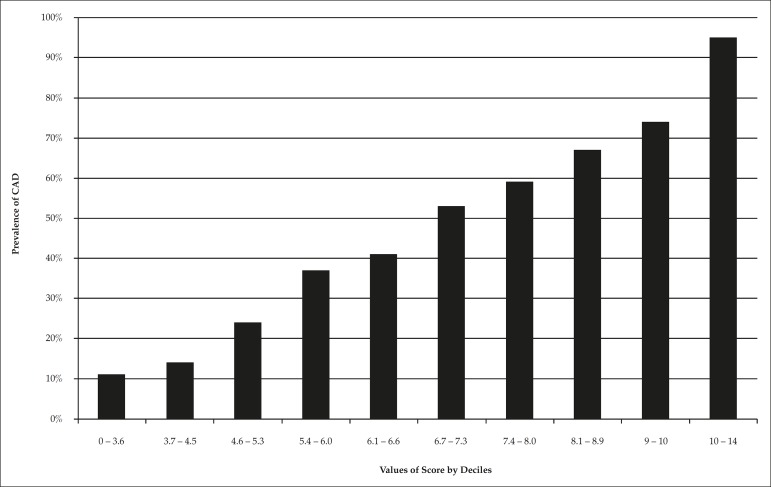
Results:: The prevalence of CAD was 48%. By logistic regression, six variables remained independent predictors of CAD: age, male gender, relief with nitrate, signs of heart failure, positive electrocardiogram, and troponin. The area under the curve (AUC) of this final model was 0.80 (95% confidence interval [95%CI] = 0.75 - 0.84) in the derivation sample and 0.86 (95%CI = 0.79 - 0.93) in the validation sample. Hosmer-Lemeshow's test indicated good calibration in both samples (p = 0.98 and p = 0.23, respectively). Compared with a basic model containing electrocardiogram and troponin, the full model provided an AUC increment of 0.07 in both derivation (p = 0.0002) and validation (p = 0.039) samples. Integrated discrimination improvement was 0.09 in both derivation (p < 0.001) and validation (p < 0.0015) samples.
Conclusion:: A multivariate model was derived and validated as an accurate tool for estimating the pretest probability of CAD in patients with acute chest pain.
Fundamento:: Atualmente, não existe um modelo multivariado validado para predizer a probabilidade de doença coronariana obstrutiva em pacientes com dor torácica aguda.
Objetivo:: Desenvolver e validar um modelo multivariado para predizer doença arterial coronariana (DAC) com base em variáveis avaliadas à admissão na unidade coronariana (UC) devido a dor torácica aguda.
Métodos:: Foram estudados um total de 470 pacientes, 370 utilizados como amostra de derivação e os subsequentes 100 pacientes como amostra de validação. Como padrão de referência, a angiografia foi necessária para descartar DAC (estenose ≥ 70%), enquanto a angiografia ou um teste não invasivo negativo foi utilizado para confirmar a doença. Foram testadas como preditoras 13 variáveis basais relacionadas à história médica, 14 características de desconforto torácico e oito variáveis relacionadas ao exame físico ou testes laboratoriais.
Resultados:: A prevalência de DAC foi de 48%. Por regressão logística, seis variáveis permaneceram como preditoras independentes de DAC: idade, gênero masculino, alívio com nitrato, sinais de insuficiência cardíaca, e eletrocardiograma e troponina positivos. A área sob a curva (area under the curve, AUC) deste modelo final foi de 0,80 (intervalo de confiança de 95% [IC95%] = 0,75 - 0,84) na amostra de derivação e 0,86 (IC95% = 0,79 - 0,93) na amostra de validação. O teste de Hosmer-Lemeshow indicou uma boa calibração em ambas as amostras (p = 0,98 e p = 0,23, respectivamente). Em comparação com o modelo básico contendo eletrocardiograma e troponina, o modelo completo ofereceu um incremento na AUC de 0,07 tanto na amostra de derivação (p = 0,0002) quanto na de validação (p = 0,039). A melhoria na discriminação integrada foi de 0,09 nas amostras de derivação (p < 0,001) e validação (p < 0,0015).
Conclusão:: Um modelo multivariado foi derivado e validado como uma ferramenta acurada para estimar a probabilidade pré-teste de DAC em pacientes com dor torácica aguda.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Amsterdam EA, Kirk JD, Bluemke DA, Diercks D, Farkouh ME, Garvey JL, et al. Testing of low-risk patients presenting to the emergency department with chest pain: A scientific statement from the american heart association. Circulation. 2010;122(17):1756–1776. on behalf of the American Heart Association Exercise CR.Prevention Committee of the Council on Clinical Cardiology CoCN.Care ICoQo.Research O. - PMC - PubMed
-
- Hermann LK, Newman DH, Pleasant W, Roianasmtikul D, Lakoff D, Goldberg AS, et al. Yield of routine provocative cardiac testing among patients in an emergency department-based chest pain unit. JAMA Intern Med. 2013;173(12):1128–1133. - PubMed
-
- Redberg RF. Coronary ct angiography for acute chest pain. N Engl J Med. 2012;367(4):375–376. - PubMed
-
- Kachalia A, Mello MM. Defensive medicine-legally necessary but ethically wrong?: Inpatient stress testing for chest pain in low-risk patients. JAMA Intern Med. 2013;173(4):1056–1057. - PubMed
-
- Pencina MJ, D' Agostino RB, D' Agostino RB, Vasan RS. Evaluating the added predictive ability of a new marker: From area under the roc curve to reclassification and beyond. Stat Med. 2008;27(2):157–172. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
