

Diffuse cystic lung diseases: differential diagnosis
- PMID: 28538782
- PMCID: PMC5474378
- DOI: 10.1590/S1806-37562016000000341
Diffuse cystic lung diseases: differential diagnosis
Abstract
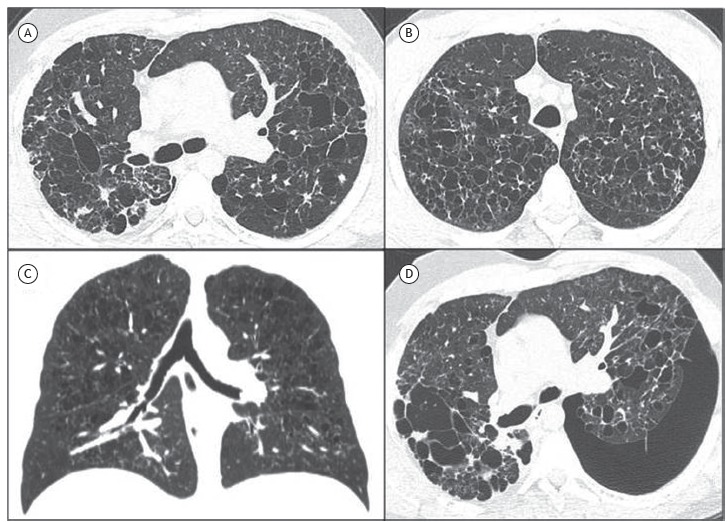
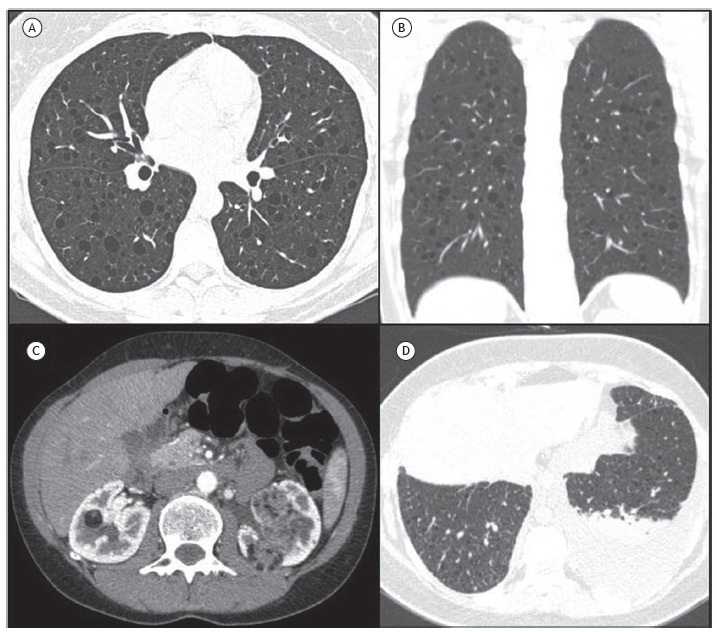
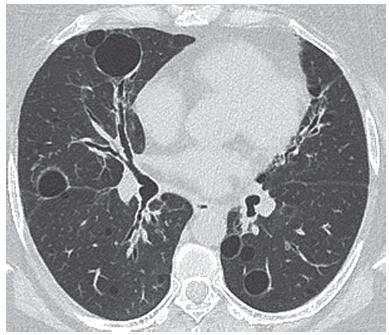
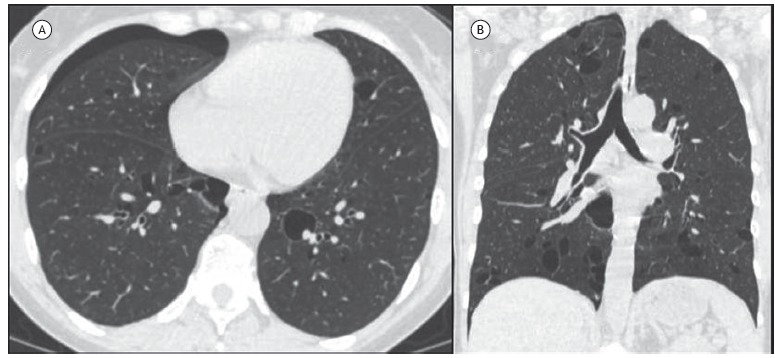
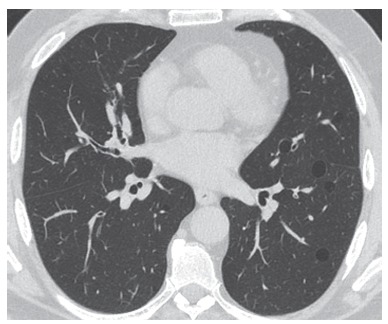
Diffuse cystic lung diseases are characterized by cysts in more than one lung lobe, the cysts originating from various mechanisms, including the expansion of the distal airspaces due to airway obstruction, necrosis of the airway walls, and parenchymal destruction. The progression of these diseases is variable. One essential tool in the evaluation of these diseases is HRCT, because it improves the characterization of pulmonary cysts (including their distribution, size, and length) and the evaluation of the regularity of the cyst wall, as well as the identification of associated pulmonary and extrapulmonary lesions. When combined with clinical and laboratory findings, HRCT is often sufficient for the etiological definition of diffuse lung cysts, avoiding the need for lung biopsy. The differential diagnoses of diffuse cystic lung diseases are myriad, including neoplastic, inflammatory, and infectious etiologies. Pulmonary Langerhans cell histiocytosis, lymphangioleiomyomatosis, lymphocytic interstitial pneumonia, and follicular bronchiolitis are the most common diseases that produce this CT pattern. However, new diseases have been included as potential determinants of this pattern. RESUMO As doenças pulmonares císticas difusas se caracterizam pela presença de cistos envolvendo mais de um lobo pulmonar, que se originam por diversos mecanismos, incluindo dilatação dos espaços aéreos distais por obstrução, necrose das paredes das vias aéreas e destruição do parênquima. Essas doenças apresentam evolução variável. A TCAR é fundamental na avaliação dessas doenças uma vez que permite uma melhor caracterização dos cistos pulmonares, incluindo sua distribuição, tamanho, extensão e regularidade das paredes, assim como a determinação de outras lesões pulmonares e extrapulmonares associadas. Frequentemente a TCAR é suficiente para a definição etiológica dos cistos pulmonares difusos, associada a achados clínicos e laboratoriais, sem a necessidade de realização de biópsia pulmonar. O diagnóstico diferencial das doenças pulmonares císticas difusas é extenso, incluindo etiologias neoplásicas, inflamatórias e infecciosas, sendo as mais frequentes determinantes desse padrão tomográfico a histiocitose pulmonar de células de Langerhans, a linfangioleiomiomatose, a pneumonia intersticial linfocitária e a bronquiolite folicular. Novas etiologias foram incluídas como potenciais determinantes desse padrão.
As doenças pulmonares císticas difusas se caracterizam pela presença de cistos envolvendo mais de um lobo pulmonar, que se originam por diversos mecanismos, incluindo dilatação dos espaços aéreos distais por obstrução, necrose das paredes das vias aéreas e destruição do parênquima. Essas doenças apresentam evolução variável. A TCAR é fundamental na avaliação dessas doenças uma vez que permite uma melhor caracterização dos cistos pulmonares, incluindo sua distribuição, tamanho, extensão e regularidade das paredes, assim como a determinação de outras lesões pulmonares e extrapulmonares associadas. Frequentemente a TCAR é suficiente para a definição etiológica dos cistos pulmonares difusos, associada a achados clínicos e laboratoriais, sem a necessidade de realização de biópsia pulmonar. O diagnóstico diferencial das doenças pulmonares císticas difusas é extenso, incluindo etiologias neoplásicas, inflamatórias e infecciosas, sendo as mais frequentes determinantes desse padrão tomográfico a histiocitose pulmonar de células de Langerhans, a linfangioleiomiomatose, a pneumonia intersticial linfocitária e a bronquiolite folicular. Novas etiologias foram incluídas como potenciais determinantes desse padrão.
Figures


Similar articles
-
Hard metal lung disease: a case series.J Bras Pneumol. 2016 Nov-Dec;42(6):447-452. doi: 10.1590/S1806-37562016000000260. J Bras Pneumol. 2016. PMID: 28117477 Free PMC article.
-
The halo sign: HRCT findings in 85 patients.J Bras Pneumol. 2016 Nov-Dec;42(6):435-439. doi: 10.1590/S1806-37562015000000029. J Bras Pneumol. 2016. PMID: 28117474 Free PMC article.
-
Impact of long-term treatment with inhaled corticosteroids and bronchodilators on lung function in a patient with post-infectious bronchiolitis obliterans.J Bras Pneumol. 2016 May-Jun;42(3):228-31. doi: 10.1590/S1806-37562016000000043. J Bras Pneumol. 2016. PMID: 27383939 Free PMC article.
-
Cardiopulmonary Exercise Test: Background, Applicability and Interpretation.Arq Bras Cardiol. 2016 Nov;107(5):467-481. doi: 10.5935/abc.20160171. Arq Bras Cardiol. 2016. PMID: 27982272 Free PMC article. Review.
-
The cerebrospinal fluid in multiple sclerosis: far beyond the bands.Einstein (Sao Paulo). 2017 Jan-Mar;15(1):100-104. doi: 10.1590/S1679-45082017RW3706. Einstein (Sao Paulo). 2017. PMID: 28444098 Free PMC article. Review.
Cited by
-
Birt-Hogg-Dubé syndrome presenting with spontaneous pneumothorax and extensive pulmonary cysts in the absence of skin lesions or renal pathology.BMJ Case Rep. 2019 Sep 6;12(9):e231039. doi: 10.1136/bcr-2019-231039. BMJ Case Rep. 2019. PMID: 31494588 Free PMC article.
-
Editorial: Advances and Updates in Diffuse Cystic Lung Diseases.Front Med (Lausanne). 2021 Jun 7;8:691688. doi: 10.3389/fmed.2021.691688. eCollection 2021. Front Med (Lausanne). 2021. PMID: 34164420 Free PMC article. No abstract available.
-
Lymphocytic interstitial pneumonia: computed tomography findings in 36 patients.Radiol Bras. 2020 Sep-Oct;53(5):287-292. doi: 10.1590/0100-3984.2019.0107. Radiol Bras. 2020. PMID: 33071371 Free PMC article.
-
Early and Atypical Radiologic Presentations of Pulmonary Langerhans Cell Histiocytosis: A Report of Two Cases.Taehan Yongsang Uihakhoe Chi. 2021 May;82(3):756-763. doi: 10.3348/jksr.2020.0061. Epub 2021 Mar 22. Taehan Yongsang Uihakhoe Chi. 2021. PMID: 36238773 Free PMC article.
-
Pulmonary mucosa-associated lymphoid tissue (MALT) lymphoma presented as cystic lung disease - a case report in Tuen Mun Hospital Hong Kong.Radiol Case Rep. 2022 Jul 27;17(10):3457-3460. doi: 10.1016/j.radcr.2022.06.064. eCollection 2022 Oct. Radiol Case Rep. 2022. PMID: 35912290 Free PMC article.
References
-
- Silva CI, Marchiori E, Souza AS, Júnior, Müller NL. Comissão de Imagem da Sociedade Brasileira de Pneumologia e Tisiologia Illustrated Brazilian consensus of terms and fundamental patterns in chest CT scans. J Bras Pneumol. 2010;36(1):99–123. https://doi.org/10.1590/S1806-37132010000100016 - DOI - PubMed
-
- Gupta N, Vassallo R, Wikenheiser-Brokamp KA, McCormack FX. Diffuse Cystic Lung Disease Part II. Am J Respir Crit Care Med. 2015;192(1):17–29. https://doi.org/10.1164/rccm.201411-2096CI - DOI - PMC - PubMed
-
- Ferreira Francisco FA, Soares Souza A, Jr, Zanetti G, Marchiori E. Multiple cystic lung disease. Eur Respir Rev. 2015;24(138):552–564. https://doi.org/10.1183/16000617.0046-2015 - DOI - PMC - PubMed
-
- Costa AN, Marchiori E, Benard G, Araújo MS, Baldi BG, Kairalla RA. Lung cysts in chronic paracoccidioidomycosis. J Bras Pneumol. 2013;39(3):368–372. https://doi.org/10.1590/S1806-37132013000300015 - DOI - PMC - PubMed
-
- Kawano-Dourado L, Baldi BG, Dias OM, Bernardi FD, Carvalho CR, Dolhnikoff M. Scattered lung cysts as the main radiographic finding of constrictive bronchiolitis. Am J Respir Crit Care Med. 2012;186(3):294–295. https://doi.org/10.1164/ajrccm.186.3.294 - DOI - PubMed
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
