

Multiparametric plasma EV profiling facilitates diagnosis of pancreatic malignancy
- PMID: 28539469
- PMCID: PMC5846089
- DOI: 10.1126/scitranslmed.aal3226
Multiparametric plasma EV profiling facilitates diagnosis of pancreatic malignancy
Abstract
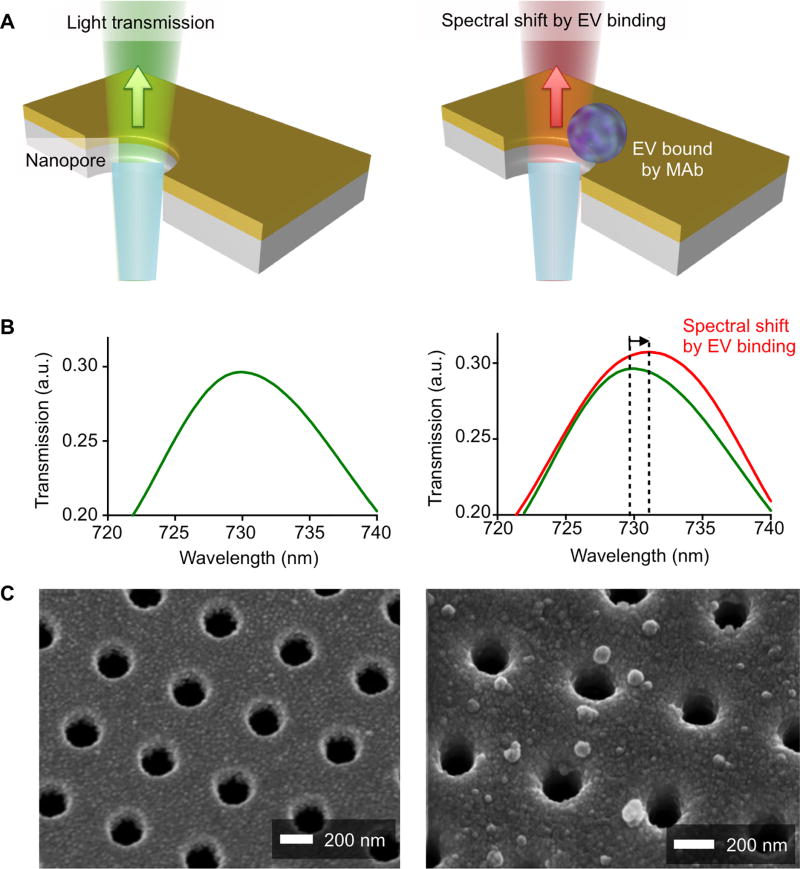
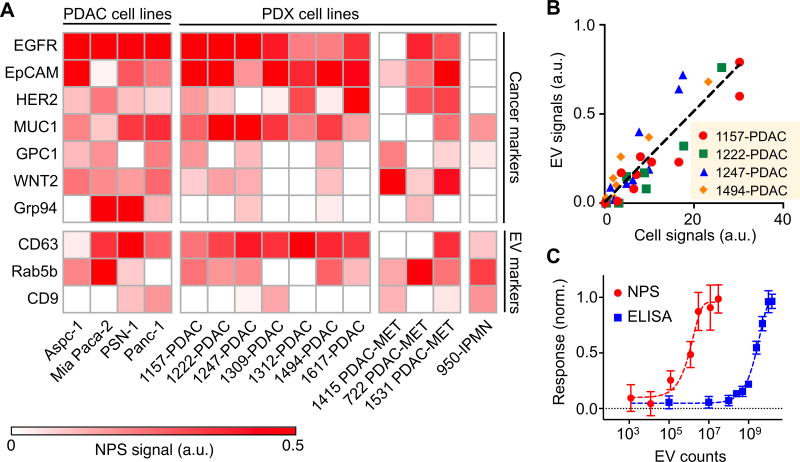
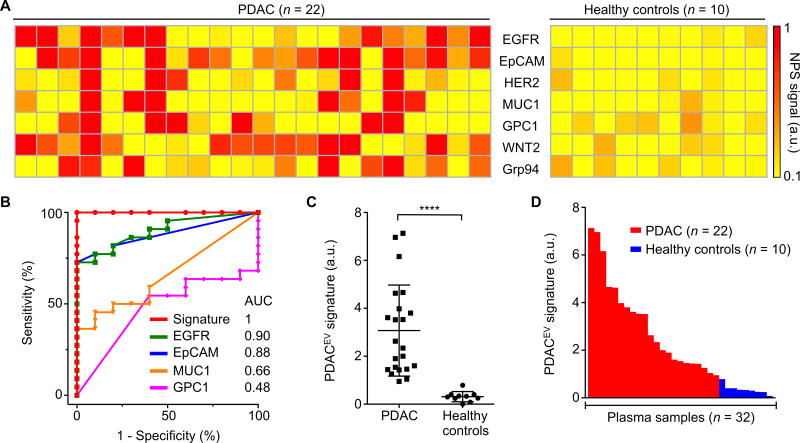
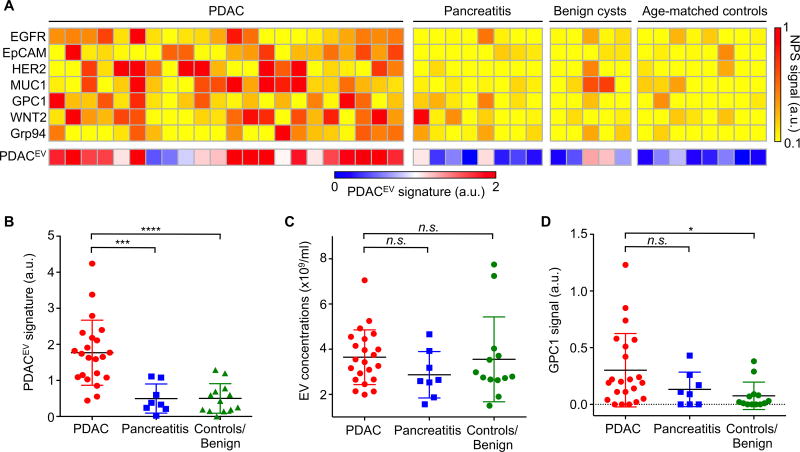
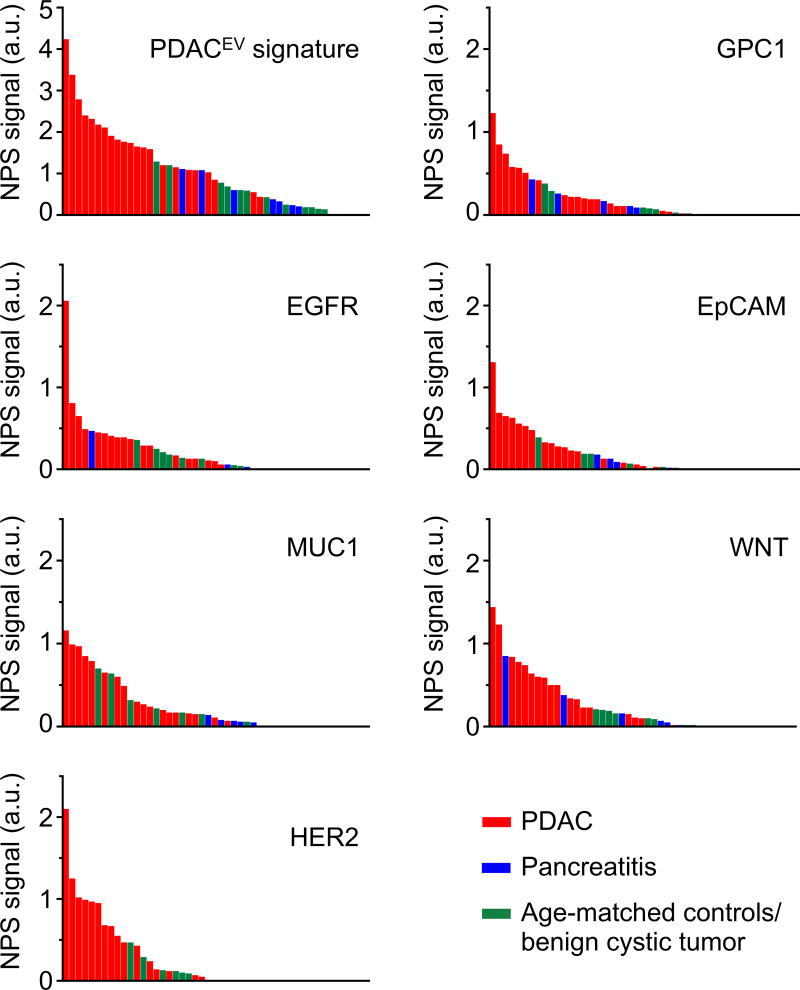
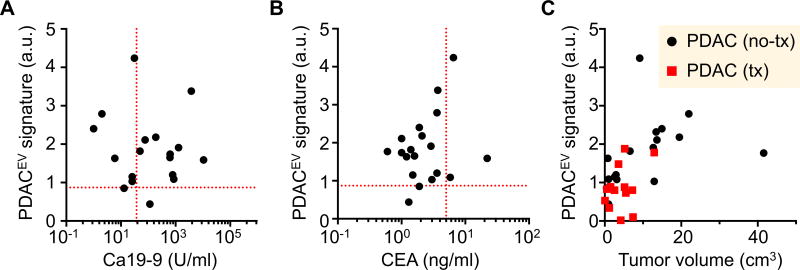
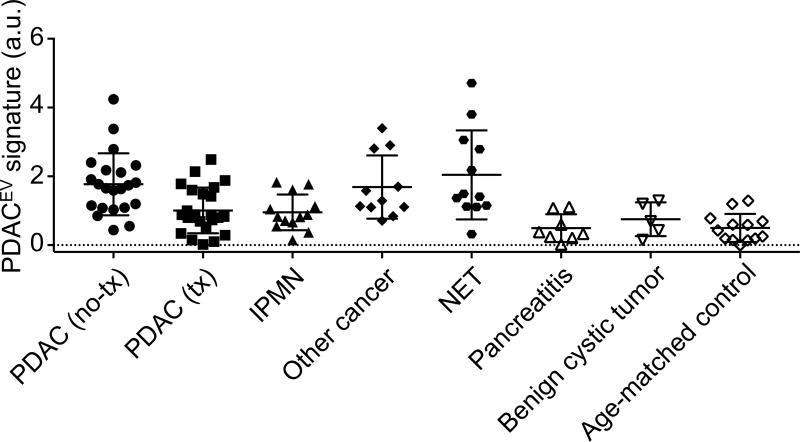
Pancreatic ductal adenocarcinoma (PDAC) is usually detected late in the disease process. Clinical workup through imaging and tissue biopsies is often complex and expensive due to a paucity of reliable biomarkers. We used an advanced multiplexed plasmonic assay to analyze circulating tumor-derived extracellular vesicles (tEVs) in more than 100 clinical populations. Using EV-based protein marker profiling, we identified a signature of five markers (PDACEV signature) for PDAC detection. In our prospective cohort, the accuracy for the PDACEV signature was 84% [95% confidence interval (CI), 69 to 93%] but only 63 to 72% for single-marker screening. One of the best markers, GPC1 alone, had a sensitivity of 82% (CI, 60 to 95%) and a specificity of 52% (CI, 30 to 74%), whereas the PDACEV signature showed a sensitivity of 86% (CI, 65 to 97%) and a specificity of 81% (CI, 58 to 95%). The PDACEV signature of tEVs offered higher sensitivity, specificity, and accuracy than the existing serum marker (CA 19-9) or single-tEV marker analyses. This approach should improve the diagnosis of pancreatic cancer.
Copyright © 2017, American Association for the Advancement of Science.
Conflict of interest statement
Figures
Comment in
-
Profiling of plasma-derived extracellular vesicles cargo for diagnosis of pancreatic malignancy.Ann Transl Med. 2017 Dec;5(24):501. doi: 10.21037/atm.2017.10.23. Ann Transl Med. 2017. PMID: 29299462 Free PMC article. No abstract available.
References
-
- Rahib L, Fleshman JM, Matrisian LM, Berlin JD. Evaluation of Pancreatic Cancer Clinical Trials and Benchmarks for Clinically Meaningful Future Trials: A Systematic Review. JAMA Oncol. 2016;2:1209–1216. - PubMed
-
- Ghatnekar O, Andersson R, Svensson M, Persson U, Ringdahl U, Zeilon P, Borrebaeck CA. Modelling the benefits of early diagnosis of pancreatic cancer using a biomarker signature. Int J Cancer. 2013;133:2392–2397. - PubMed
-
- Duffy MJ, Sturgeon C, Lamerz R, Haglund C, Holubec VL, Klapdor R, Nicolini A, Topolcan O, Heinemann V. Tumor markers in pancreatic cancer: a European Group on Tumor Markers (EGTM) status report. Ann Oncol. 2010;21:441–447. - PubMed
-
- Seufferlein T, Mayerle J. Pancreatic cancer in 2015: Precision medicine in pancreatic cancer--fact or fiction. Nat Rev Gastroenterol Hepatol. 2016;13:74–75. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
