

Successful withdrawal from high-dose benzodiazepine in a young patient through electronic monitoring of polypharmacy: a case report in an ambulatory setting
- PMID: 28540039
- PMCID: PMC5431399
- DOI: 10.1177/2045125317690502
Successful withdrawal from high-dose benzodiazepine in a young patient through electronic monitoring of polypharmacy: a case report in an ambulatory setting
Abstract
Background: Dependence on high-dose benzodiazepines (BZDs) is well known and discontinuation attempts are generally unsuccessful. A well established protocol for high-dose BZD withdrawal management is lacking. We present the case of withdrawal from high-dose lorazepam (>20 mg daily) in an unemployed 35-year-old male outpatient through agonist substitution with long-acting clonazepam and electronic monitoring over 28 weeks.
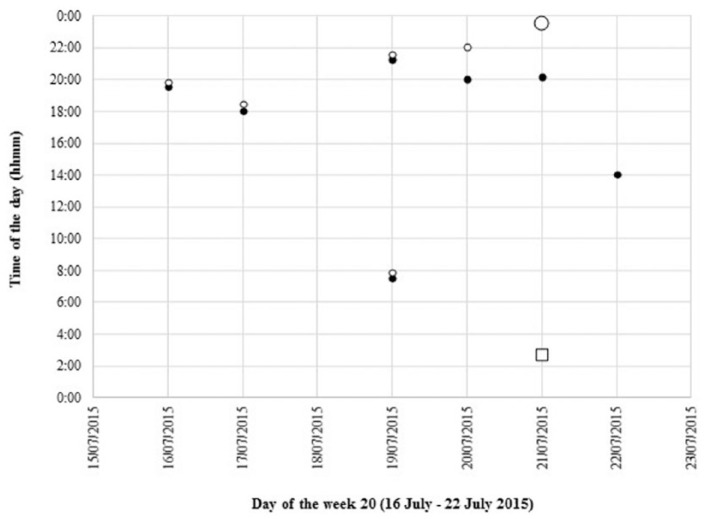
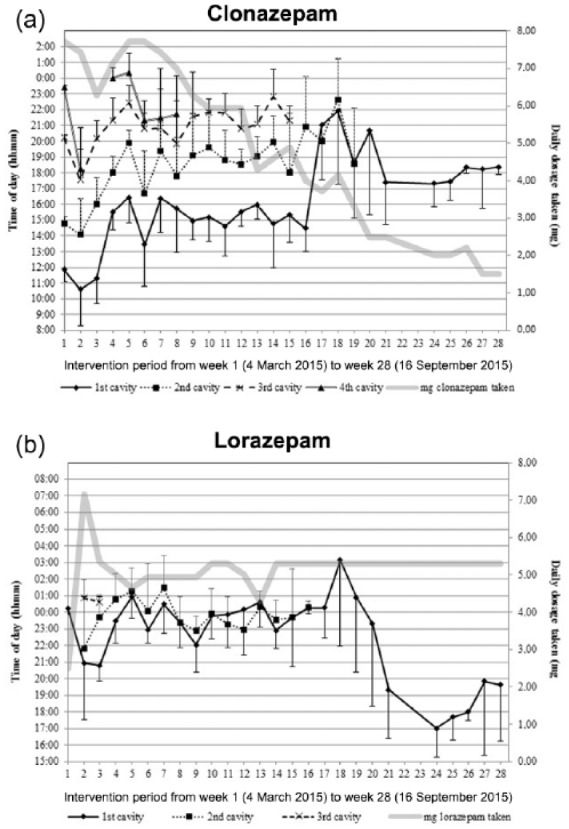
Methods: All medicines were repacked into weekly 7 × 4 cavity multidose punch cards with an electronic monitoring system. The prescribed daily dosages of BZDs were translated into an optimal number of daily tablets, divided into up to four units of use. Withdrawal was achieved by individual leftover of a small quantity of BZDs that was placed in a separate compartment. Feedback with visualization of intake over the past week was given during weekly psychosocial sessions.
Results: Stepwise reduction was obtained by reducing the mg content of the cavities proportionally to the leftovers, keeping the number of cavities in order to maintain regular intake behavior, and to determine the dosage decrease. At week 28, the primary objectives were achieved, that is, lorazepam reduction to 5 mg daily and cannabis abstinence. Therapy was continued using multidrug punch cards without electronic monitoring to maintain the management system. At week 48, a smaller size weekly pill organizer with detachable daily containers was dispensed. At week 68, the patient's therapy was constant with 1.5 mg clonazepam + 5 mg lorazepam daily for anxiety symptoms and the last steps of withdrawal were started.
Conclusions: Several key factors led to successful withdrawal from high-dose BZD in this outpatient, such as the use of weekly punch cards coupled with electronic monitoring, the patient's empowerment over the withdrawal process, and the collaboration of several healthcare professionals. The major implication for clinical care is reduction by following the leftovers, and not a diktat from the healthcare professionals.
Keywords: addiction; benzodiazepine; community pharmacy; electronic monitoring; multidrug punch card; printed electronics; substance withdrawal.
Conflict of interest statement
Conflict of interest statement: The authors declare that there is no conflict of interest.
Figures
Similar articles
-
Successful Rapid Benzodiazepine Detoxification in an Acute Care Hospital: A Case Report.J Community Hosp Intern Med Perspect. 2024 Jul 2;14(4):93-96. doi: 10.55729/2000-9666.1373. eCollection 2024. J Community Hosp Intern Med Perspect. 2024. PMID: 39391115 Free PMC article.
-
[In utero exposure to benzodiazepine. Is there a risk for anal atresia with lorazepam?].Encephale. 2003 Nov-Dec;29(6):553-9. Encephale. 2003. PMID: 15029090 Review. French.
-
Multidrug punch cards in primary care: a mixed methods study on patients' preferences and impact on adherence.Front Pharmacol. 2014 Oct 1;5:220. doi: 10.3389/fphar.2014.00220. eCollection 2014. Front Pharmacol. 2014. PMID: 25324777 Free PMC article.
-
Reasons for Benzodiazepine Use Among Persons Seeking Opioid Detoxification.J Subst Abuse Treat. 2016 Sep;68:57-61. doi: 10.1016/j.jsat.2016.06.008. Epub 2016 Jun 16. J Subst Abuse Treat. 2016. PMID: 27431047 Free PMC article.
-
Benzodiazepine dependence and withdrawal: identification and medical management.J Am Board Fam Pract. 1992 Mar-Apr;5(2):167-75. J Am Board Fam Pract. 1992. PMID: 1575069 Review.
Cited by
-
Comprehensive evaluation of flumazenil adverse reactions: Insights from FAERS data and signal detection algorithms.Medicine (Baltimore). 2025 Mar 7;104(10):e41721. doi: 10.1097/MD.0000000000041721. Medicine (Baltimore). 2025. PMID: 40068036 Free PMC article.
-
Physicians' beliefs and attitudes about Benzodiazepines: a cross-sectional study.BMC Fam Pract. 2019 May 25;20(1):71. doi: 10.1186/s12875-019-0965-0. BMC Fam Pract. 2019. PMID: 31128589 Free PMC article.
References
-
- Lader M. History of benzodiazepine dependence. J Subst Abuse Treat 1991; 8: 53–59. - PubMed
-
- O’Brien C. Benzodiazepine use, abuse, and dependence. J Clin Psychiatry 2005; 66(Suppl. 2): 28–33. - PubMed
-
- Petitjean S, Ladewig D, Meier CR, et al. Benzodiazepine prescribing to the Swiss adult population: results from a national survey of community pharmacies. Int Clin Psychopharmacol 2007; 22: 292–298. - PubMed
-
- Lagnaoui R, Depont F, Fourrier A, et al. Patterns and correlates of benzodiazepine use in the French general population. Eur J Clin Pharmacol 2004; 60: 523–529. - PubMed
-
- Windle A, Elliot E, Duszynski K, et al. Benzodiazepine prescribing in elderly Australian general practice patients. Aust N Z J Public Health 2007; 31: 379–381. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
