

Trends in the Management of Patients With Kidney Failure in Alberta, Canada (2004-2013)
- PMID: 28540058
- PMCID: PMC5433679
- DOI: 10.1177/2054358117698668
Trends in the Management of Patients With Kidney Failure in Alberta, Canada (2004-2013)
Abstract
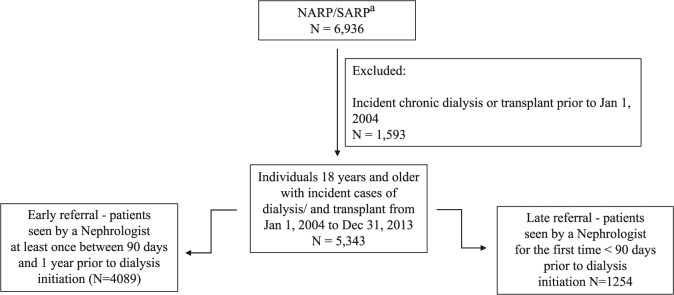
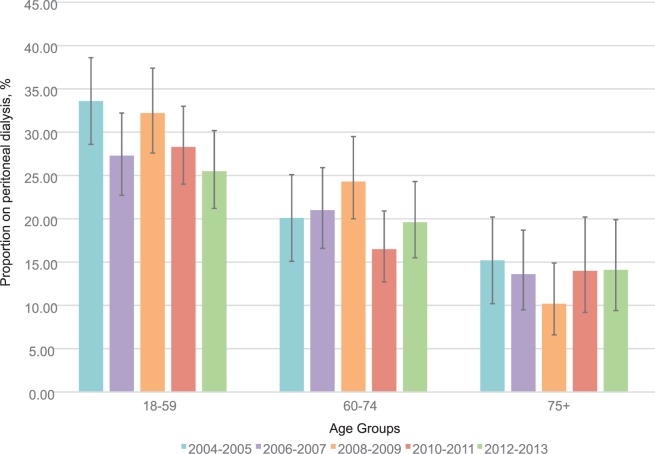
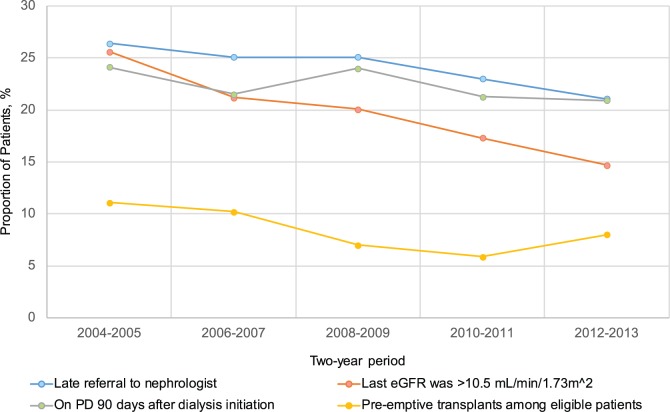
Background: Based on clinical practice guidelines, specific quality indicators are examined to assess the performance of a health care system for patients with end-stage renal disease (ESRD). We examined trends in the proportion of patients with ESRD referred late to nephrology, timing of dialysis initiation in those with chronic kidney disease, and proportion of patients with ESRD treated with pre-emptive kidney transplantation or peritoneal dialysis (PD). Design:: This was a retrospective cohort study. Setting:: The study was conducted in Alberta, Canada. Patients:: Alberta residents aged 18 years or older with incident ESRD requiring renal replacement therapy between 2004 and 2013 were included. Measurements:: Descriptive statistics, and log binomial and linear regression models were used for analysis. Methods:: We determined the proportion of patients with ESRD who did not see a nephrologist within 90 days prior to starting dialysis (late referrals) and those who were receiving PD 90 days after dialysis initiation. Among those who had been seen by a nephrologist for at least 90 days, we also assessed the proportion who initiated dialysis with estimated glomerular filtration rate (eGFR) higher than or equal to 10.5 mL/min/1.73 m2, and underwent a pre-emptive transplant. Results:: Our cohort included 5343 patients (mean age 61.8 years, 61.2% male). Over a 10-year period, there was a decrease in the proportion of late referrals (26.4% to 21.1%, P = .001). We also noted a decrease in the proportion of dialysis initiation with eGFR higher than or equal to 10.5 mL/min/1.73 m2 (21.2% to 14.7%, P < .001), with a significant increase in the proportion of patients initiating dialysis as an inpatient (38.8% to 45.2%, P = .001). There was a non-significant decrease in both the proportion of patients treated with a pre-emptive transplant and PD at 90 days over the 10-year period. Limitations:: The use of administrative data restricted the availability of clinical data regarding underlying circumstances of each quality indicator, including patient symptoms, indications for dialysis initiation, and PD eligibility.
Conclusions: We noted improvement in late referrals and early dialysis initiation over time. However, we also noted low and stable use of pre-emptive kidney transplantation and PD at 90 days, which warrants further exploration. These findings support the need for quality improvement initiatives designed to address these gaps in care and improve outcomes for patients with kidney failure.
Mise en contexte: Les indicateurs de la qualité, lorsqu’ils s’appuient sur des preuves solides, permettent d’évaluer efficacement la performance d’un système de soins de santé, y compris les soins dispensés aux patients atteints d’insuffisance rénale terminale (IRT). Nous avons examiné les tendances en matière d’indicateurs de la qualité, y compris la proportion de patients orientés tardivement en néphrologie, ainsi que la proportion de patients traités par dialyse péritonéale (DP) ou au moyen d’une greffe de rein comme modalité initiale de remplacement de la fonction rénale.
Type d’étude: Il s’agit d’une étude de cohorte rétrospective.
Cadre: L’étude a été menée en Alberta, au Canada.
Patients: Il s’agit de patients albertains adultes nouvellement atteints d’IRT et nécessitant une thérapie continue de remplacement rénal.
Mesures: Nous avons mesuré la proportion de patients qui n’avait pas vu un néphrologue dans les 90 jours précédant l’amorce de la dialyse (orientation tardive) ; la proportion de patients chez qui on avait amorcé la dialyse à la suite d’une mesure du DFGe ≥ 10.5 mL/min/1.73 m2 et la proportion de patients qui avaient subi une greffe comme modalité initiale de thérapie de remplacement de la fonction rénale et la proportion de ceux qui étaient traités par DP à 90 jours.
Méthodologie: Nous avons utilisé des statistiques descriptives, un modèle logarithmique binomial ainsi que des modèles de régression linéaire pour évaluer les tendances des indicateurs de la qualité mentionnés ci-dessus.
Résultats: Notre cohorte était formée de 5343 patients (61,2 % d’hommes) dont l’âge moyen se situait à 61.8 ans. Sur une période de 10 ans, nous avons observé que la proportion d’orientations tardives est passée de 26.4% à 21.1% (P = .001). Nous avons aussi noté une diminution de la proportion de patients chez qui on avait amorcé la dialyse avec une mesure du DFGe ≥ 10.5 mL/min/1.73 m2 (21.2% à 14.7%, P < .001). Toutefois, nous avons constaté une augmentation significative de la proportion de patients chez qui la dialyse avait été amorcée lors d’une hospitalisation (38.8% à 45.2%, P = .001). Enfin, nous avons noté une diminution non significative dans la proportion de patients traités par une greffe comme modalité initiale de remplacement de la fonction rénale ainsi que dans la proportion des patients traités par DP à 90 jours au cours de la même période.
Limites de l’étude: L’utilisation de données administratives a limité la disponibilité des données cliniques en ce qui concerne les circonstances sous-jacentes à chaque indicateur de la qualité, incluant les symptômes du patient, les indications pour l’initiation de la dialyse et l’admissibilité à la dialyse péritonéale.
Conclusions: Nous avons constaté une amélioration en ce qui concerne les orientations tardives et l’initiation d’une dialyse précoce au fil du temps. Cependant, nous avons remarqué, de façon constante dans le temps, un faible recours à la transplantation rénale comme modalité initiale et à la DP à 90 jours, ce qui devrait faire l’objet d’une étude plus poussée. Ces constatations constituent la première étape d’une proposition pour l’amélioration de la qualité conçue pour réduire les écarts observés au niveau des soins, et visant à améliorer les résultats pour les patients atteints d’insuffisance rénale.
Keywords: chronic; health care; kidney failure; kidney transplantation; peritoneal dialysis; quality indicators; renal replacement therapy.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
[REIN Report 2011--summary].Nephrol Ther. 2013 Sep;9 Suppl 1:S3-6. doi: 10.1016/S1769-7255(13)70036-1. Nephrol Ther. 2013. PMID: 24119584 French.
-
Starting Dialysis on Time, At Home on the Right Therapy (START): Description of an Intervention to Increase the Safe and Effective Use of Peritoneal Dialysis.Can J Kidney Health Dis. 2021 Mar 31;8:20543581211003764. doi: 10.1177/20543581211003764. eCollection 2021. Can J Kidney Health Dis. 2021. PMID: 33868692 Free PMC article.
-
Association Between the Publication of the Initiating Dialysis Early and Late Trial and the Timing of Dialysis Initiation in Canada.JAMA Intern Med. 2019 Jul 1;179(7):934-941. doi: 10.1001/jamainternmed.2019.0489. JAMA Intern Med. 2019. PMID: 31135821 Free PMC article. Clinical Trial.
-
Pre-emptive kidney transplantation to improve survival in patients with type 1 diabetes and imminent risk of ESRD.Semin Nephrol. 2012 Sep;32(5):505-11. doi: 10.1016/j.semnephrol.2012.07.014. Semin Nephrol. 2012. PMID: 23062992 Review.
-
Consequences of late referral on patient outcomes.Nephrol Dial Transplant. 2000;15 Suppl 3:8-13. doi: 10.1093/oxfordjournals.ndt.a027977. Nephrol Dial Transplant. 2000. PMID: 11032351 Review.
Cited by
-
Association between change in physician remuneration and use of peritoneal dialysis: a population-based cohort analysis.CMAJ Open. 2020 Feb 18;8(1):E96-E104. doi: 10.9778/cmajo.20190132. Print 2020 Jan-Mar. CMAJ Open. 2020. PMID: 32071144 Free PMC article.
References
-
- The Canadian Institute for Health Information. Canadian Organ Replacement Register Annual Report: Treatment of End-Stage Organ Failure in Canada, 2004 to 2013. Ottawa, Ontario: Canadian Institution for Health Information; 2015.
-
- Collins AJ, Foley RN, Gilbertson DT, Chen S-C. The state of chronic kidney disease, ESRD, and morbidity and mortality in the first year of dialysis. Clin J Am Soc Nephrol. 2009;4(suppl 1):S5-S11. - PubMed
-
- Foley RN, Murray AM, Li S, et al. Chronic kidney disease and the risk for cardiovascular disease, renal replacement, and death in the United States Medicare population, 1998 to 1999. J Am Soc Nephrol. 2005;16(2):489-495. - PubMed
-
- Mix TCH, St. Peter WL, Ebben J, et al. Hospitalization during advancing chronic kidney disease. Am J Kidney Dis. 2003;42(5):972-981. - PubMed
-
- Manns BJ, Mendelssohn DC, Taub KJ. The economics of end-stage renal disease care in Canada: incentives and impact on delivery of care. Int J Health Care Finance Econ. 2007;7(2):149-169. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
