

Presurgical role of MRI tractography in a case of extensive cervicothoracic spinal ependymoma
- PMID: 28540122
- PMCID: PMC5421221
- DOI: 10.4103/sni.sni_33_17
Presurgical role of MRI tractography in a case of extensive cervicothoracic spinal ependymoma
Abstract
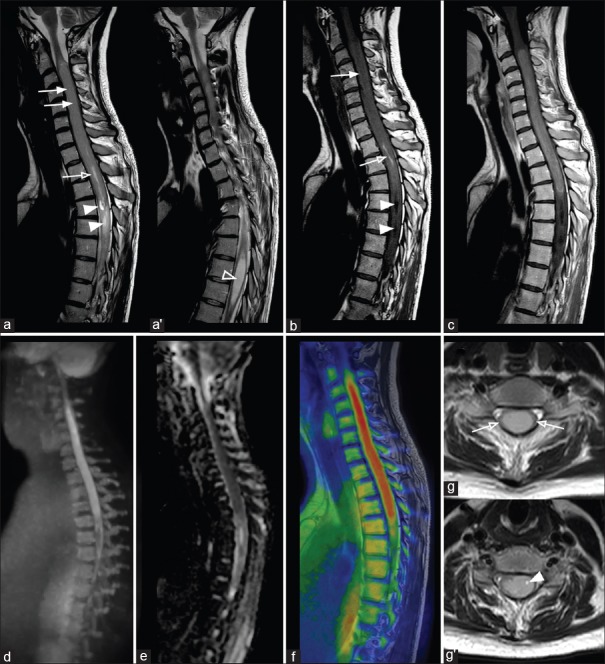
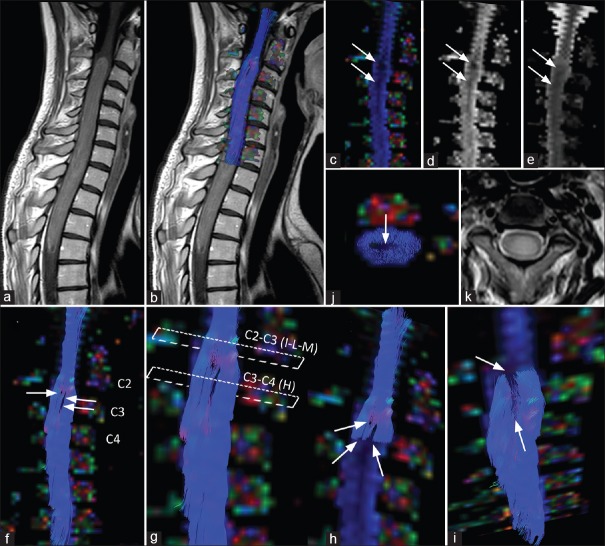
Background: Intramedullary spinal ependymoma is a tumor, hardly characterizable with conventional magnetic resonance (MR) imaging only. MR diffusion tensor imaging (DTI) with three-dimensional fiber-tracking reconstructions allows the evaluation of the relationship between neoplasm and white matter fiber tracts, being a powerful tool in presurgical planning. We present DTI findings in a case of a young female with an extensive cervicothoracic spinal ependymoma.
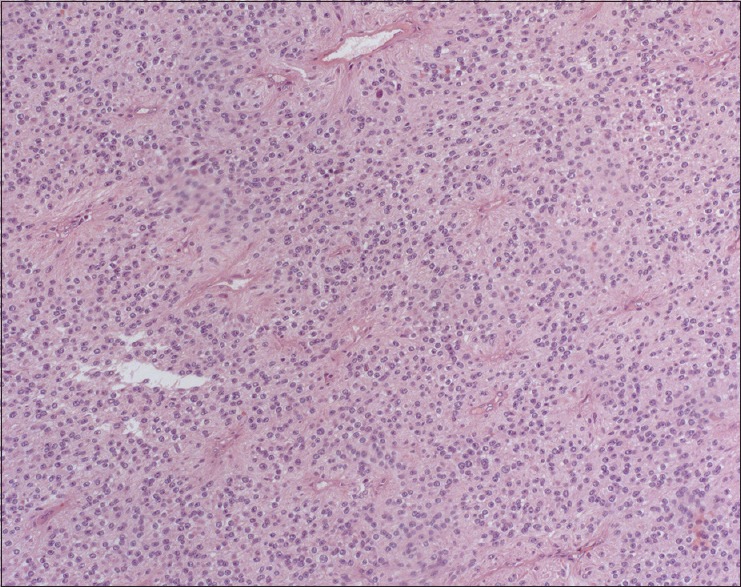
Case description: The patient complained of a 2-month history of acute urinary retention, weakness and numbness on the lower limbs and the upper left limb. She underwent MR imaging that showed an extensive cervicothoracic spinal mass, difficult to characterize with conventional MR sequences. DTI showed peripherally displacement of fibers, without involvement of the spinal cord, findings consistent with an ependymoma. The patient underwent surgery with a complete resection "en bloc" of the lesion, which showed clear cleavage planes, as detected by DTI. Histopathological findings confirmed the diagnosis of ependymoma.
Conclusions: DTI is a useful tool in presurgical planning, helping in differentiating not infiltrating neoplasms, such as spinal ependymomas, from other infiltrative and more aggressive neoplasms, which are considered not resectable.
Keywords: Cervicothoracic tract; DTI; ependymoma; spinal cord.
Conflict of interest statement
There are no conflicts of interest.
Figures
Similar articles
-
Combined Use of Diffusion Tractography and Advanced Intraoperative Imaging for Resection of Cervical Intramedullary Spinal Cord Neoplasms: A Case Series and Technical Note.Oper Neurosurg. 2019 Nov 1;17(5):525-530. doi: 10.1093/ons/opz039. Oper Neurosurg. 2019. PMID: 30892657
-
Microsurgery resection of giant cervicothoracic spinal ependymoma: Two-dimensional operative video.Surg Neurol Int. 2024 Jul 12;15:237. doi: 10.25259/SNI_317_2024. eCollection 2024. Surg Neurol Int. 2024. PMID: 39108377 Free PMC article.
-
Spinal diffusion tensor tractography for differentiation of intramedullary tumor-suspected lesions.Eur J Radiol. 2016 Dec;85(12):2275-2280. doi: 10.1016/j.ejrad.2016.10.018. Epub 2016 Oct 17. Eur J Radiol. 2016. PMID: 27842677
-
Remarkable efficacy of temozolomide for relapsed spinal myxopapillary ependymoma with multiple recurrence and cerebrospinal dissemination: a case report and literature review.Eur Spine J. 2018 Jul;27(Suppl 3):421-425. doi: 10.1007/s00586-017-5413-z. Epub 2017 Dec 21. Eur Spine J. 2018. PMID: 29270703 Review.
-
Prognosis by tumor location in adults with spinal ependymomas.J Neurosurg Spine. 2013 Mar;18(3):226-35. doi: 10.3171/2012.12.SPINE12591. Epub 2013 Jan 11. J Neurosurg Spine. 2013. PMID: 23311515 Review.
Cited by
-
Sodium Fluorescein for Spinal Intradural Tumors.Front Oncol. 2021 Jan 28;10:618579. doi: 10.3389/fonc.2020.618579. eCollection 2020. Front Oncol. 2021. PMID: 33585245 Free PMC article.
-
Surgical approaches to intramedullary spinal cord astrocytomas in the age of genomics.Front Oncol. 2022 Sep 6;12:982089. doi: 10.3389/fonc.2022.982089. eCollection 2022. Front Oncol. 2022. PMID: 36147920 Free PMC article. Review.
-
Full cervical cord tractography: A new method for clinical use.Front Neuroanat. 2022 Sep 27;16:993464. doi: 10.3389/fnana.2022.993464. eCollection 2022. Front Neuroanat. 2022. PMID: 36237419 Free PMC article.
-
The use of diffusion tensor imaging in spinal pathology: a comprehensive literature review.Eur Spine J. 2024 Sep;33(9):3303-3314. doi: 10.1007/s00586-024-08231-8. Epub 2024 Jul 16. Eur Spine J. 2024. PMID: 39014075 Review.
References
-
- Chimelli L. Tumors and tumor like lesions of the spine and spinal cord. Neuroimaging Clin N Am. 2001;11:79–110. - PubMed
-
- Ducreux D, Fillard P, Facon D, Ozanne A, Lepeintre JF, Renoux J, et al. Diffusion tensor magnetic resonance imaging and fiber tracking in spinal cord lesions: Current and future indications. Neuroimaging Clin N Am. 2007;17:137–47. - PubMed
-
- Egger K, Hohenhaus M, Van Velthoven V, Heil S, Urbach H. Spinal diffusion tensor tractography for differentiation of intramedullary tumor-suspected lesions. Eur J Radiol. 2016;85:2275–80. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials