

Evidence-based Utilization of Noninvasive Ventilation and Patient Outcomes
- PMID: 28541747
- PMCID: PMC5711281
- DOI: 10.1513/AnnalsATS.201703-208OC
Evidence-based Utilization of Noninvasive Ventilation and Patient Outcomes
Abstract
Rationale: Strong evidence supports use of noninvasive ventilation (NIV) for patients with respiratory distress from chronic obstructive pulmonary disease and heart failure (strong evidence conditions [SECs]). Despite unclear benefits of NIV for other causes of acute respiratory failure, utilization for conditions with weaker evidence is increasing, despite evidence demonstrating higher mortality for patients who suffer NIV failure (progression from NIV to invasive mechanical ventilation [IMV])) compared with being treated initially with IMV.
Objectives: To determine the association of hospital variation in evidence-based utilization of NIV with patient outcomes.
Methods: Using the California State Inpatient Database 2011, we identified adult patients who received NIV. Patients were considered to have an SEC for NIV if they had an acute exacerbation of chronic obstructive pulmonary disease or heart failure. We used multivariable hierarchical logistic regression to determine the association between hospital rates of NIV use for SECs and patient risk of NIV failure (need for IMV after NIV).
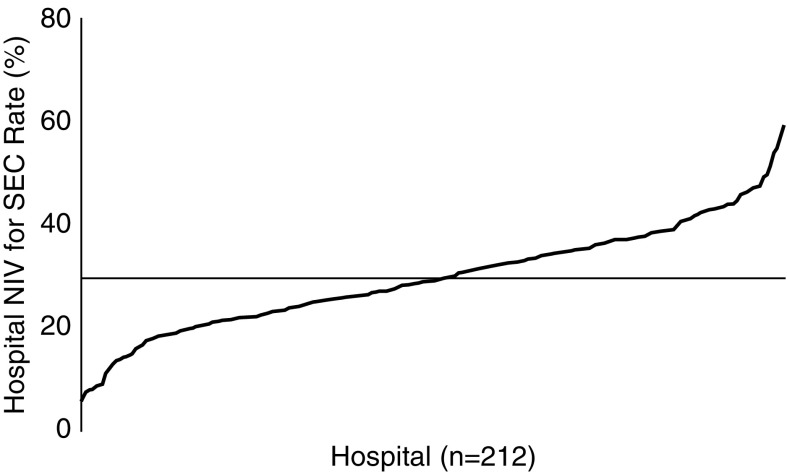
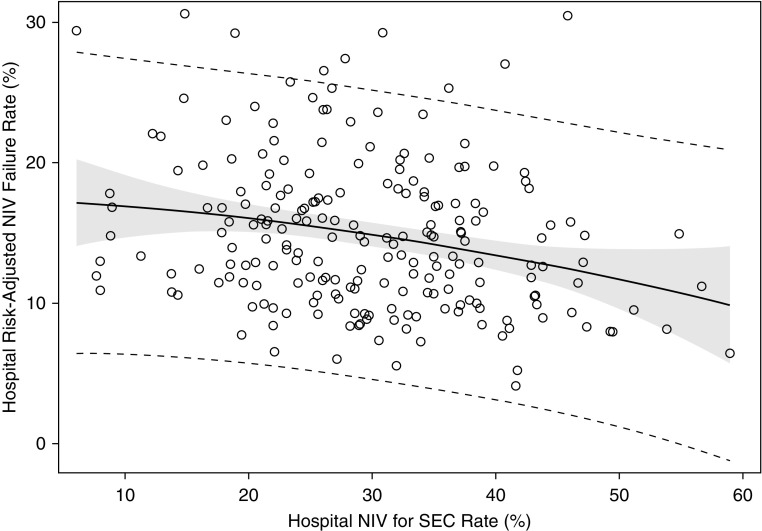
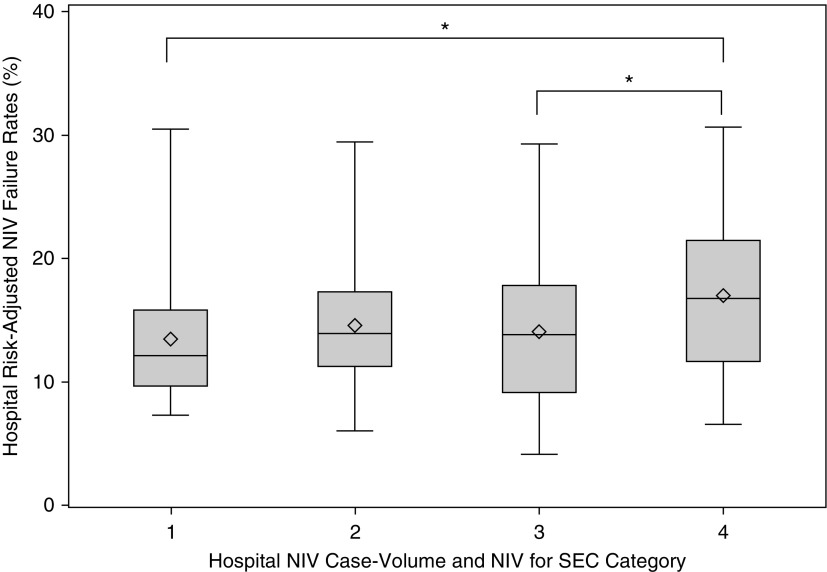
Results: Among 22,706 hospitalizations with NIV as the initial ventilatory strategy, 6,820 (30.0%) had SECs. Patients with SECs had lower risk of NIV failure than patients with weak evidence conditions (8.1 vs. 18.2%, P < 0.0001). Regardless of underlying diagnosis, patients admitted to hospitals with greater use of NIV for SECs had lower risk of NIV failure (Quartile 4 vs. Quartile 1 adjusted odds ratio = 0.62; 95% CI = 0.49-0.80). Even patients without an SEC benefited from admission to hospitals that used NIV more often for patients with SECs (Quartile 4 vs. Quartile 1 adjusted odds ratio for NIV failure = 0.68; 95% CI = 0.52-0.88).
Conclusions: Most patients who received NIV did not have conditions with strong supporting evidence for its use with wide institutional variation in patient selection for NIV. Surprisingly, we found that all patients, even those without an SEC, benefited from admission to hospitals with greater evidence-based utilization of NIV, suggesting a "hospital effect" that is synergistic with patient selection.
Keywords: chronic obstructive pulmonary disease; heart failure; invasive mechanical ventilation; noninvasive ventilation.
Figures
Comment in
-
Noninvasive Ventilation across Hospitals: An Example of Healthcare Delivery Science.Ann Am Thorac Soc. 2017 Nov;14(11):1634-1635. doi: 10.1513/AnnalsATS.201706-470ED. Ann Am Thorac Soc. 2017. PMID: 29090991 No abstract available.
Similar articles
-
Hospital Noninvasive Ventilation Case Volume and Outcomes of Acute Exacerbations of Chronic Obstructive Pulmonary Disease.Ann Am Thorac Soc. 2016 Oct;13(10):1752-1759. doi: 10.1513/AnnalsATS.201603-209OC. Ann Am Thorac Soc. 2016. PMID: 27404021 Free PMC article.
-
Outcomes of Noninvasive and Invasive Ventilation in Patients Hospitalized with Asthma Exacerbation.Ann Am Thorac Soc. 2016 Jul;13(7):1096-104. doi: 10.1513/AnnalsATS.201510-701OC. Ann Am Thorac Soc. 2016. PMID: 27070493 Free PMC article.
-
Use of noninvasive ventilation in patients with acute respiratory failure, 2000-2009: a population-based study.Ann Am Thorac Soc. 2013 Feb;10(1):10-7. doi: 10.1513/AnnalsATS.201206-034OC. Ann Am Thorac Soc. 2013. PMID: 23509327 Free PMC article.
-
Management of Chronic Respiratory Failure in Chronic Obstructive Pulmonary Disease: High-Intensity and Low-Intensity Ventilation.Sleep Med Clin. 2020 Dec;15(4):497-509. doi: 10.1016/j.jsmc.2020.08.007. Sleep Med Clin. 2020. PMID: 33131660 Review.
-
Epidemiology of NIV for Acute Respiratory Failure in COPD Patients: Results from the International Surveys vs. the "Real World".COPD. 2017 Aug;14(4):429-438. doi: 10.1080/15412555.2017.1336527. Epub 2017 Jun 21. COPD. 2017. PMID: 28636452 Review.
Cited by
-
The Association of Frailty With Long-Term Outcomes in Patients With Acute Respiratory Failure Treated With Noninvasive Ventilation.Cureus. 2022 Dec 30;14(12):e33143. doi: 10.7759/cureus.33143. eCollection 2022 Dec. Cureus. 2022. PMID: 36726891 Free PMC article.
-
Characteristics and Risk Factors for Mortality in Critically Ill Patients with COVID-19 Receiving Invasive Mechanical Ventilation: The Experience of a Private Network in Sao Paulo, Brazil.J Crit Care Med (Targu Mures). 2022 Aug 12;8(3):165-175. doi: 10.2478/jccm-2022-0015. eCollection 2022 Jul. J Crit Care Med (Targu Mures). 2022. PMID: 36062038 Free PMC article.
-
Noninvasive Ventilation for Critically Ill Subjects With Acute Respiratory Failure in the Emergency Department.Respir Care. 2020 Jan;65(1):82-90. doi: 10.4187/respcare.07111. Epub 2019 Oct 1. Respir Care. 2020. PMID: 31575708 Free PMC article.
-
Hospital Variation in Renal Replacement Therapy for Sepsis in the United States.Crit Care Med. 2018 Feb;46(2):e158-e165. doi: 10.1097/CCM.0000000000002878. Crit Care Med. 2018. PMID: 29206766 Free PMC article.
-
ICU Utilization for Patients With Acute Exacerbation of Chronic Obstructive Pulmonary Disease Receiving Noninvasive Ventilation.Crit Care Med. 2019 May;47(5):677-684. doi: 10.1097/CCM.0000000000003660. Crit Care Med. 2019. PMID: 30720540 Free PMC article.
References
-
- Brochard L, Mancebo J, Wysocki M, Lofaso F, Conti G, Rauss A, Simonneau G, Benito S, Gasparetto A, Lemaire F, et al. Noninvasive ventilation for acute exacerbations of chronic obstructive pulmonary disease. N Engl J Med. 1995;333:817–822. - PubMed
-
- Plant PK, Owen JL, Elliott MW. Early use of non-invasive ventilation for acute exacerbations of chronic obstructive pulmonary disease on general respiratory wards: a multicentre randomised controlled trial. Lancet. 2000;355:1931–1935. - PubMed
-
- Conti G, Antonelli M, Navalesi P, Rocco M, Bufi M, Spadetta G, Meduri GU. Noninvasive vs. conventional mechanical ventilation in patients with chronic obstructive pulmonary disease after failure of medical treatment in the ward: a randomized trial. Intensive Care Med. 2002;28:1701–1707. - PubMed
-
- Ram FS, Picot J, Lightowler J, Wedzicha JA. Non-invasive positive pressure ventilation for treatment of respiratory failure due to exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2004;(3):CD004104. - PubMed
-
- Peter JV, Moran JL, Phillips-Hughes J, Graham P, Bersten AD. Effect of non-invasive positive pressure ventilation (NIPPV) on mortality in patients with acute cardiogenic pulmonary oedema: a meta-analysis. Lancet. 2006;367:1155–1163. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
