

Subsidies for Oral Chemotherapy and Use of Immunomodulatory Drugs Among Medicare Beneficiaries With Myeloma
- PMID: 28541791
- PMCID: PMC5652870
- DOI: 10.1200/JCO.2017.72.2447
Subsidies for Oral Chemotherapy and Use of Immunomodulatory Drugs Among Medicare Beneficiaries With Myeloma
Abstract
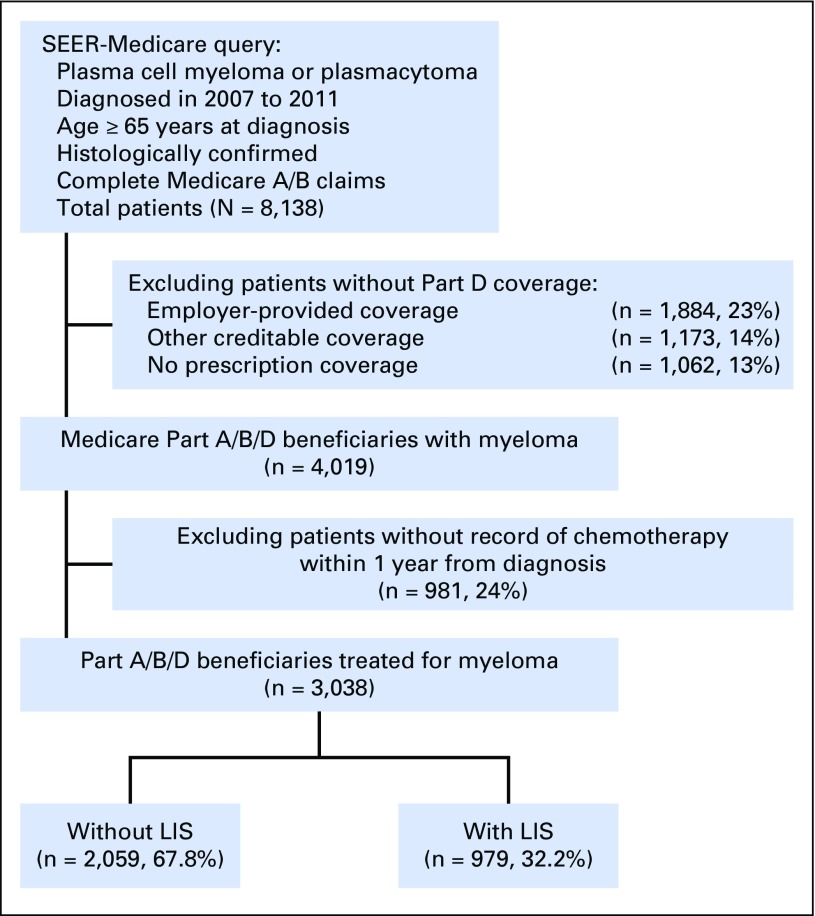
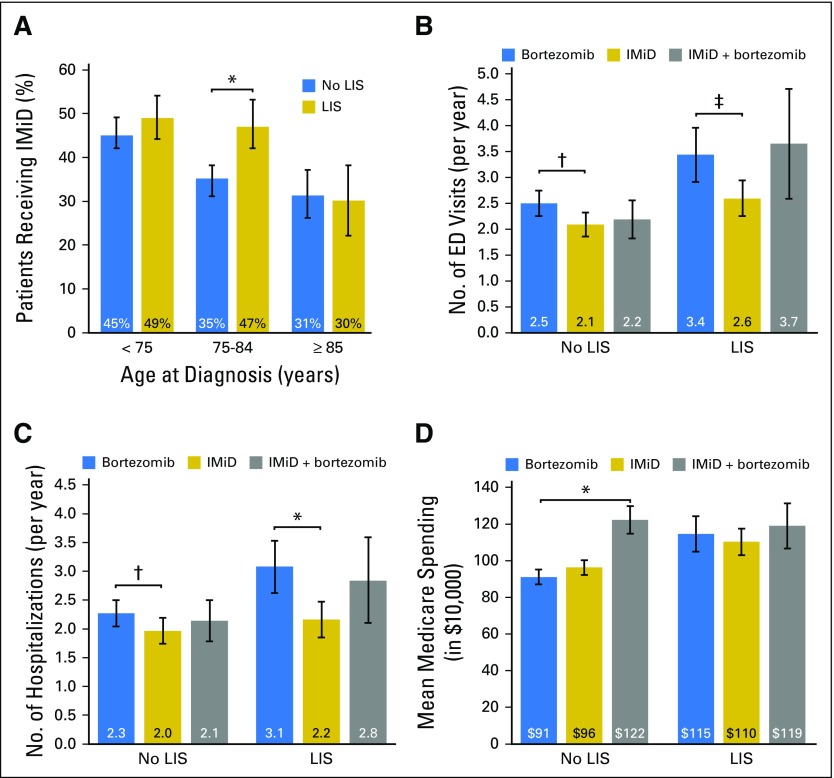
Purpose The low-income subsidy (LIS) substantially lowers out-of-pocket costs for qualifying Medicare Part D beneficiaries who receive orally administered chemotherapy. We examined the association of LIS with the use of novel oral immunomodulatory drugs (IMiDs; lenalidomide and thalidomide) among beneficiaries with myeloma, who can receive either orally administered or parenteral (bortezomib-based) therapy. Methods Using SEER-Medicare data, we identified Part D beneficiaries diagnosed with myeloma in 2007 to 2011. In multivariable models adjusted for sociodemographic and clinical characteristics, we analyzed associations between the LIS and use of IMiD-based therapy, delays between IMiD refills, and select health outcomes during the first year of therapy. Results Among 3,038 beneficiaries, 41% received first-line IMiDs. Median out-of-pocket cost for the first IMiD prescription was $3,178 for LIS nonrecipients and $3 for LIS recipients, whereas the respective median costs for the first year of therapy were $5,623 and $6, respectively. Receipt of the LIS was associated with a 32% higher (95% CI, 16% to 47%) probability of receiving IMiDs among beneficiaries age 75 to 84 years and a significantly lower risk of delays between refills in all age groups (adjusted relative risk, 0.54; 95% CI, 0.32 to 0.92). Duration of therapy did not significantly differ between LIS recipients and nonrecipients (median, 7.6 months). Patients treated with IMiDs had significantly fewer emergency department visits and hospitalizations compared with patients receiving bortezomib (without IMiDs), but 1-year overall survival and cumulative Medicare costs were similar. Conclusion Medicare beneficiaries with myeloma who do not receive LISs face a substantial financial barrier to accessing orally administered anticancer therapy, warranting urgent attention from policymakers. Limiting out-of-pocket costs for expensive anticancer drugs like the IMiDs may improve access to oral therapy for patients with myeloma.
Figures
References
-
- Facon T, Mary JY, Hulin C, et al. : Melphalan and prednisone plus thalidomide versus melphalan and prednisone alone or reduced-intensity autologous stem cell transplantation in elderly patients with multiple myeloma (IFM 99-06): A randomised trial. Lancet 370:1209-1218, 2007 - PubMed
-
- Palumbo A, Bringhen S, Liberati AM, et al. : Oral melphalan, prednisone, and thalidomide in elderly patients with multiple myeloma: Updated results of a randomized controlled trial. Blood 112:3107-3114, 2008 - PubMed
-
- Mateos MV, Richardson PG, Schlag R, et al. : Bortezomib plus melphalan and prednisone compared with melphalan and prednisone in previously untreated multiple myeloma: Updated follow-up and impact of subsequent therapy in the phase III VISTA trial. J Clin Oncol 28:2259-2266, 2010 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
