

Treatment with enalapril and not diltiazem ameliorated progression of chronic kidney disease in rats, and normalized renal AT1 receptor expression as measured with PET imaging
- PMID: 28542215
- PMCID: PMC5438116
- DOI: 10.1371/journal.pone.0177451
Treatment with enalapril and not diltiazem ameliorated progression of chronic kidney disease in rats, and normalized renal AT1 receptor expression as measured with PET imaging
Abstract
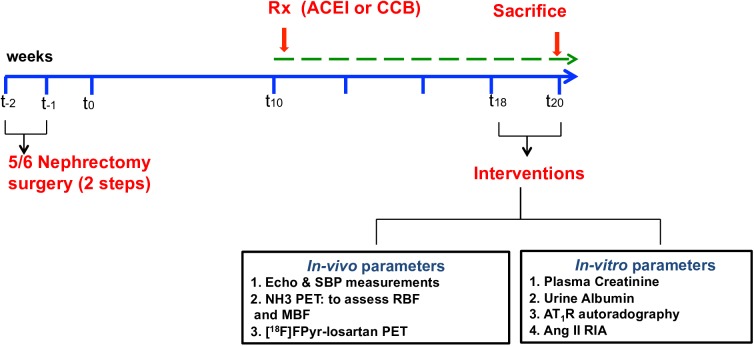
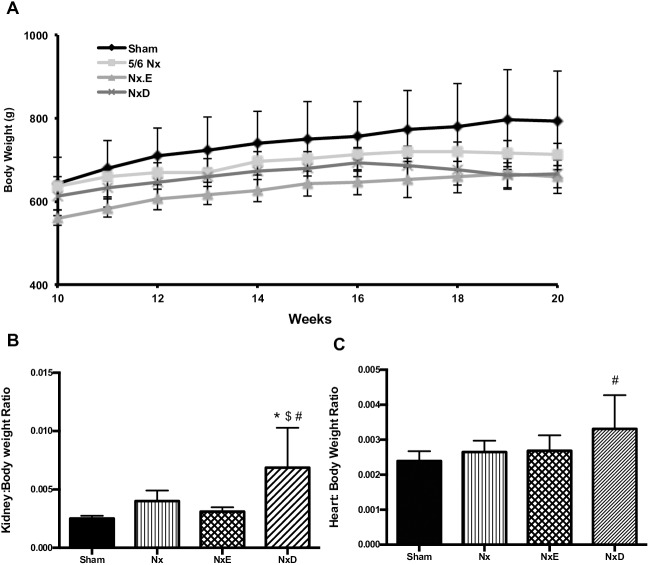
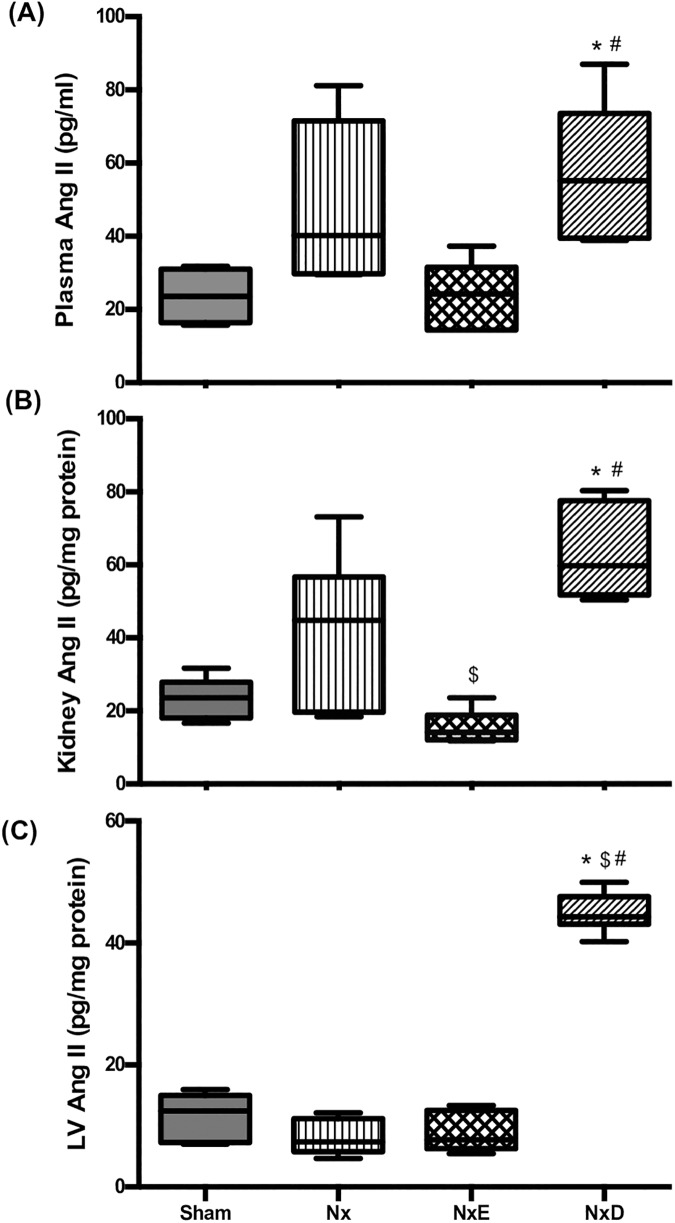
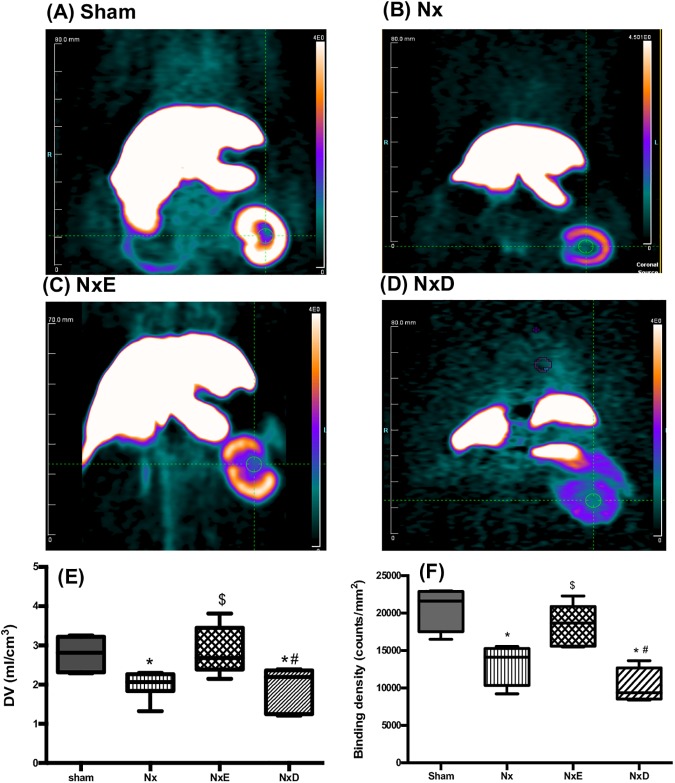
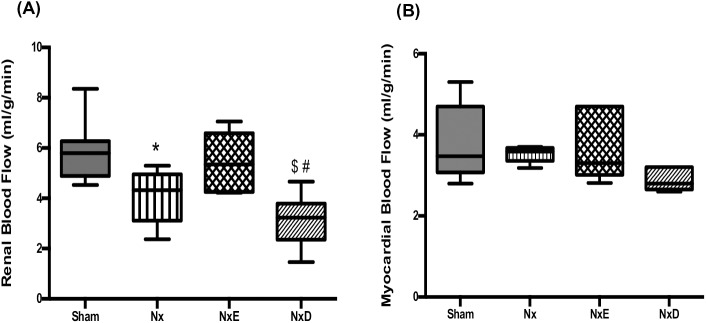
ACE inhibitors are considered first line of treatment in patients with many forms of chronic kidney disease (CKD). Other antihypertensives such as calcium channel blockers achieve similar therapeutic effectiveness in attenuating hypertension-related renal damage progression. Our objective was to explore the value of positron emission tomography (PET) imaging of renal AT1 receptor (AT1R) to guide therapy in the 5/6 subtotal-nephrectomy (Nx) rat model of CKD. Ten weeks after Nx, Sprague-Dawley rats were administered 10mg/kg/d enalapril (NxE), 30mg/kg/d diltiazem (NxD) or left untreated (Nx) for an additional 8-10 weeks. Kidney AT1R expression was assessed using in vivo [18F]fluoropyridine-losartan PET and in vitro autoradiography. Compared to shams, Nx rats exhibited higher systolic blood pressure that was reduced by both enalapril and diltiazem. At 18-20 weeks, plasma creatinine and albuminuria were significantly increased in Nx, reduced to sham levels in NxE, but enhanced in NxD rats. Enalapril treatment decreased kidney angiotensin II whereas diltiazem induced significant elevations in plasma and kidney levels. Reduced PET renal AT1R levels in Nx were normalized by enalapril but not diltiazem, and results were supported by autoradiography. Reduction of renal blood flow in Nx was restored by enalapril, while no difference was observed in myocardial blood flow amongst groups. Enhanced left ventricle mass in Nx was not reversed by enalapril but was augmented with diltiazem. Stroke volume was diminished in untreated Nx compared to shams and restored with both therapies. [18F]Fluoropyridine-Losartan PET allowed in vivo quantification of kidney AT1R changes associated with progression of CKD and with various pharmacotherapies.
Conflict of interest statement
Figures
Similar articles
-
Enalapril in subantihypertensive dosage attenuates kidney proliferation and functional recovery in normotensive ablation nephropathy of the rat.Physiol Res. 1999;48(6):429-35. Physiol Res. 1999. PMID: 10783907
-
Enalapril inhibits growth and proliferation of various tissues in rat normotensive four-sixths kidney ablation nephropathy.Kidney Blood Press Res. 2000;23(2):106-12. doi: 10.1159/000025961. Kidney Blood Press Res. 2000. PMID: 10765112
-
Vitamin D receptor agonist VS-105 improves cardiac function in the presence of enalapril in 5/6 nephrectomized rats.Am J Physiol Renal Physiol. 2015 Feb 15;308(4):F309-19. doi: 10.1152/ajprenal.00129.2014. Epub 2014 Dec 10. Am J Physiol Renal Physiol. 2015. PMID: 25503724 Free PMC article.
-
[Molecular mechanisms of nephro-protective action of enalapril in experimental chronic renal failure].Ann Acad Med Stetin. 1999;Suppl 52:1-93. Ann Acad Med Stetin. 1999. PMID: 10589103 Review. Polish.
-
Diltiazem: ten years of clinical experience in the treatment of hypertension.J Clin Pharmacol. 1995 Mar;35(3):220-32. doi: 10.1002/j.1552-4604.1995.tb04051.x. J Clin Pharmacol. 1995. PMID: 7608309 Review.
Cited by
-
Novel 18F-Labeled PET Imaging Agent FV45 Targeting the Renin-Angiotensin System.ACS Omega. 2018 Sep 30;3(9):10460-10470. doi: 10.1021/acsomega.8b01885. Epub 2018 Sep 4. ACS Omega. 2018. PMID: 30288456 Free PMC article.
-
Synthesis of the Novel AT1 Receptor Tracer [18F]Fluoropyridine-Candesartan via Click Chemistry.ACS Omega. 2020 Aug 3;5(32):20353-20362. doi: 10.1021/acsomega.0c02310. eCollection 2020 Aug 18. ACS Omega. 2020. PMID: 32832788 Free PMC article.
-
Non-invasive molecular imaging of kidney diseases.Nat Rev Nephrol. 2021 Oct;17(10):688-703. doi: 10.1038/s41581-021-00440-4. Epub 2021 Jun 29. Nat Rev Nephrol. 2021. PMID: 34188207 Free PMC article. Review.
-
Medicinal (Radio) Chemistry: Building Radiopharmaceuticals for the Future.Curr Med Chem. 2024;31(34):5481-5534. doi: 10.2174/0929867331666230818092634. Curr Med Chem. 2024. PMID: 37594105 Review.
References
-
- Levin A, Hemmelgarn B, Culleton B, Tobe S, McFarlane P, Ruzicka M et al.: Guidelines for the management of chronic kidney disease. CMAJ. 2008;179:1154–62. doi: 10.1503/cmaj.080351 - DOI - PMC - PubMed
-
- Arora P, Vasa P, Brenner D, Iglar K, McFarlane P, Morrison H et al.: Prevalence estimates of chronic kidney disease in Canada: results of a nationally representative survey. CMAJ. 2013;185:E417–23. doi: 10.1503/cmaj.120833 - DOI - PMC - PubMed
-
- Appel LJ, Wright JT Jr., Greene T, Agodoa LY, Astor BC, Bakris GL et al.: Intensive blood-pressure control in hypertensive chronic kidney disease. N Engl J Med. 2010;363:918–29. doi: 10.1056/NEJMoa0910975 - DOI - PMC - PubMed
-
- Pohl MA, Blumenthal S, Cordonnier DJ, De Alvaro F, Deferrari G, Eisner G et al.: Independent and additive impact of blood pressure control and angiotensin II receptor blockade on renal outcomes in the irbesartan diabetic nephropathy trial: clinical implications and limitations. J Am Soc Nephrol. 2005;16:3027–37. doi: 10.1681/ASN.2004110919 - DOI - PubMed
-
- Asselbergs FW, Diercks GF, Hillege HL, van Boven AJ, Janssen WM, Voors AA et al.: Effects of fosinopril and pravastatin on cardiovascular events in subjects with microalbuminuria. Circulation. 2004;110:2809–16. doi: 10.1161/01.CIR.0000146378.65439.7A - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
