

Inflammatory biomarkers as predictors of heart failure in women without obstructive coronary artery disease: A report from the NHLBI-sponsored Women's Ischemia Syndrome Evaluation (WISE)
- PMID: 28542263
- PMCID: PMC5438124
- DOI: 10.1371/journal.pone.0177684
Inflammatory biomarkers as predictors of heart failure in women without obstructive coronary artery disease: A report from the NHLBI-sponsored Women's Ischemia Syndrome Evaluation (WISE)
Abstract
Background: Women with signs and symptoms of ischemia, no obstructive coronary artery disease (CAD) and preserved left ventricular ejection fraction (EF) often have diastolic dysfunction and experience elevated rates of major adverse cardiac events (MACE), including heart failure (HF) hospitalization with preserved ejection fraction (HFpEF). We evaluated the predictive value of inflammatory biomarkers for long-term HF hospitalization and all-cause mortality in these women.
Methods: We performed a cross-sectional analysis to investigate the relationships between inflammatory biomarkers [serum interleukin-6 (IL-6), C-reactive protein (hs-CRP) and serum amyloid A (SAA)] and median of 6 years follow-up for all-cause mortality and HF hospitalization among women with signs and symptoms of ischemia, non-obstructive CAD and preserved EF. Multivariable Cox regression analysis tested associations between biomarker levels and adverse outcomes.
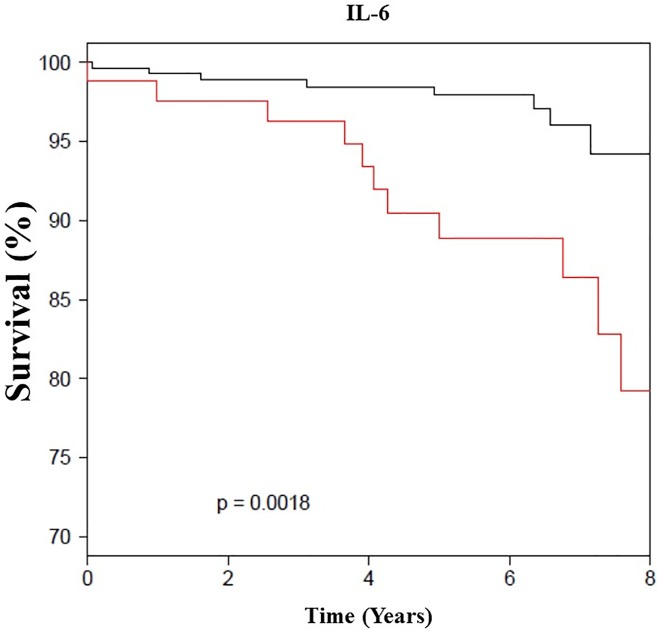
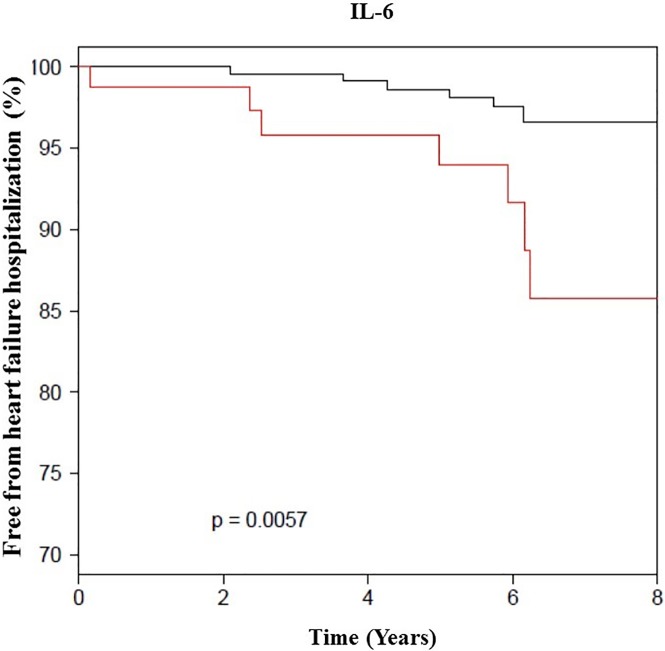
Results: Among 390 women, mean age 56 ± 11 years, median follow up of 6 years, we observed that there is continuous association between IL-6 level and HF hospitalization (adjusted hazard ratio [AHR] 2.5 [1.2-5.0], p = 0.02). In addition, we found significant association between IL-6, SAA levels and all-cause mortality AHR (1.8 [1.1-3.0], p = 0.01) (1.5 [1.0-2.1], p = 0.04), respectively.
Conclusion: In women with signs and symptoms of ischemia, non-obstructive CAD and preserved EF, elevated IL-6 predicted HF hospitalization and all-cause mortality, while SAA level was only associated with all-cause mortality. These results suggest that inflammation plays a role in the pathogenesis of development of HFpEF, as well all-cause mortality.
Conflict of interest statement
Figures
Similar articles
-
Heart failure hospitalization in women with signs and symptoms of ischemia: A report from the women's ischemia syndrome evaluation study.Int J Cardiol. 2016 Nov 15;223:936-939. doi: 10.1016/j.ijcard.2016.07.301. Epub 2016 Aug 12. Int J Cardiol. 2016. PMID: 27589041 Free PMC article.
-
Adverse outcomes among women presenting with signs and symptoms of ischemia and no obstructive coronary artery disease: findings from the National Heart, Lung, and Blood Institute-sponsored Women's Ischemia Syndrome Evaluation (WISE) angiographic core laboratory.Am Heart J. 2013 Jul;166(1):134-41. doi: 10.1016/j.ahj.2013.04.002. Epub 2013 May 2. Am Heart J. 2013. PMID: 23816032 Free PMC article. Clinical Trial.
-
Multimarker approach predicts adverse cardiovascular events in women evaluated for suspected ischemia: results from the National Heart, Lung, and Blood Institute-sponsored Women's Ischemia Syndrome Evaluation.Clin Cardiol. 2009 May;32(5):244-50. doi: 10.1002/clc.20454. Clin Cardiol. 2009. PMID: 19452486 Free PMC article.
-
Even "WISE-R?"-an Update on the NHLBI-Sponsored Women's Ischemia Syndrome Evaluation.Curr Atheroscler Rep. 2020 Jun 18;22(8):35. doi: 10.1007/s11883-020-00852-w. Curr Atheroscler Rep. 2020. PMID: 32556630 Free PMC article. Review.
-
Stable angina in women: lessons from the National Heart, Lung and Blood Institute-sponsored Women’s Ischemia Syndrome Evaluation.J Cardiovasc Med (Hagerstown). 2011 Feb;12(2):85-7. doi: 10.2459/JCM.0b013e3283430969. J Cardiovasc Med (Hagerstown). 2011. PMID: 21228716 Review.
Cited by
-
Novel biomarkers associated with incident heart failure in 10 106 Finnish men.ESC Heart Fail. 2021 Feb;8(1):605-614. doi: 10.1002/ehf2.13132. Epub 2020 Dec 5. ESC Heart Fail. 2021. PMID: 33660951 Free PMC article.
-
Shared Genetic Characteristics of Coronary Artery Disease and Peripheral artery Disease: Insights From Integrated Bioinformatics Analysis of RNA-Sequencing Data.Bioinform Biol Insights. 2025 Jun 15;19:11779322251344123. doi: 10.1177/11779322251344123. eCollection 2025. Bioinform Biol Insights. 2025. PMID: 40535026 Free PMC article.
-
Beyond the Obstructive Paradigm: Unveiling the Complex Landscape of Nonobstructive Coronary Artery Disease.J Clin Med. 2024 Aug 7;13(16):4613. doi: 10.3390/jcm13164613. J Clin Med. 2024. PMID: 39200755 Free PMC article. Review.
-
Risk Factors Predisposing to Angina in Patients with Non-Obstructive Coronary Arteries: A Retrospective Analysis.J Pers Med. 2022 Jun 27;12(7):1049. doi: 10.3390/jpm12071049. J Pers Med. 2022. PMID: 35887545 Free PMC article.
-
Molecular Hallmarks of Ischemia with Non-Obstructive Coronary Arteries: The "INOCA versus Obstructive CCS" Challenge.J Clin Med. 2022 Mar 19;11(6):1711. doi: 10.3390/jcm11061711. J Clin Med. 2022. PMID: 35330036 Free PMC article.
References
-
- Marroquin OC, Kip KE, Mulukutla SR, Ridker PM, Pepine CJ, Tjandrawan T, et al. Inflammation, endothelial cell activation, and coronary microvascular dysfunction in women with chest pain and no obstructive coronary artery disease. American heart journal. 2005;150(1):109–15. Epub 2005/08/09. doi: 10.1016/j.ahj.2004.08.003 - DOI - PubMed
-
- Pai JK, Pischon T, Ma J, Manson JE, Hankinson SE, Joshipura K, et al. Inflammatory markers and the risk of coronary heart disease in men and women. The New England journal of medicine. 2004;351(25):2599–610. Epub 2004/12/17. doi: 10.1056/NEJMoa040967 - DOI - PubMed
-
- Gulati M, Cooper-DeHoff RM, McClure C, Johnson BD, Shaw LJ, Handberg EM, et al. Adverse cardiovascular outcomes in women with nonobstructive coronary artery disease: a report from the Women's Ischemia Syndrome Evaluation Study and the St James Women Take Heart Project. Archives of internal medicine. 2009;169(9):843–50. Epub 2009/05/13. PubMed Central PMCID: PMCPMC2782882. doi: 10.1001/archinternmed.2009.50 - DOI - PMC - PubMed
-
- Bakir M, Nelson MD, Jones E, Li Q, Wei J, Sharif B, et al. Heart failure hospitalization in women with signs and symptoms of ischemia: A report from the women's ischemia syndrome evaluation study. International journal of cardiology. 2016;223:936–9. Epub 2016/09/03. doi: 10.1016/j.ijcard.2016.07.301 - DOI - PMC - PubMed
-
- Vilaro HT JR, cooper-DeHoff RM, HAndberg E, Sopko G, Kelsey S, Bairey Merz CN, Pepine CJ. Brachial Pulse Pressure Predicts Adverse Outcomes Including Heart Failure Hospitalizations in Women with Preserved Ejection Fraction and No Obstructive Coronary Artery Disease: A report from the Women’s Ischimia Syndrome Evaluation. Circulation. 2014;2014; 130(A11580).
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
