

Detecting infection hotspots: Modeling the surveillance challenge for elimination of lymphatic filariasis
- PMID: 28542274
- PMCID: PMC5453617
- DOI: 10.1371/journal.pntd.0005610
Detecting infection hotspots: Modeling the surveillance challenge for elimination of lymphatic filariasis
Abstract
Background: During the past 20 years, enormous efforts have been expended globally to eliminate lymphatic filariasis (LF) through mass drug administration (MDA). However, small endemic foci (microfoci) of LF may threaten the presumed inevitable decline of infections after MDA cessation. We conducted microsimulation modeling to assess the ability of different types of surveillance to identify microfoci in these settings.
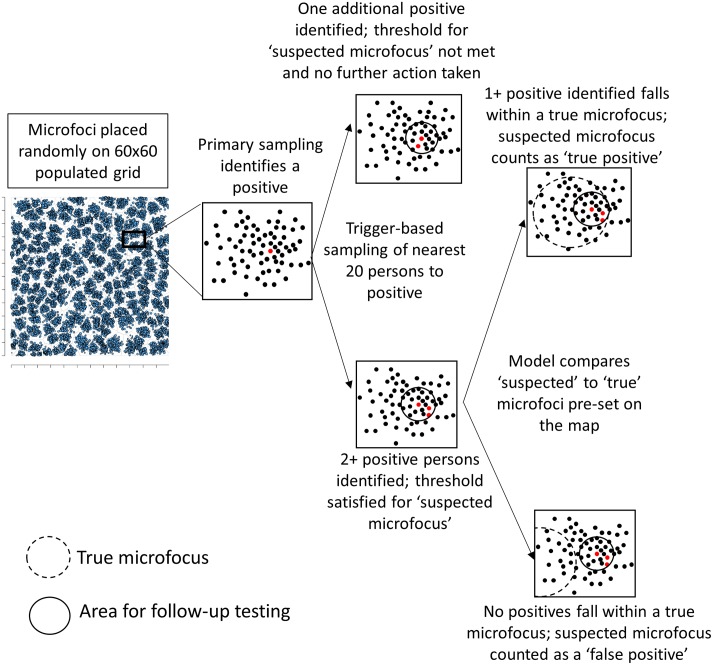
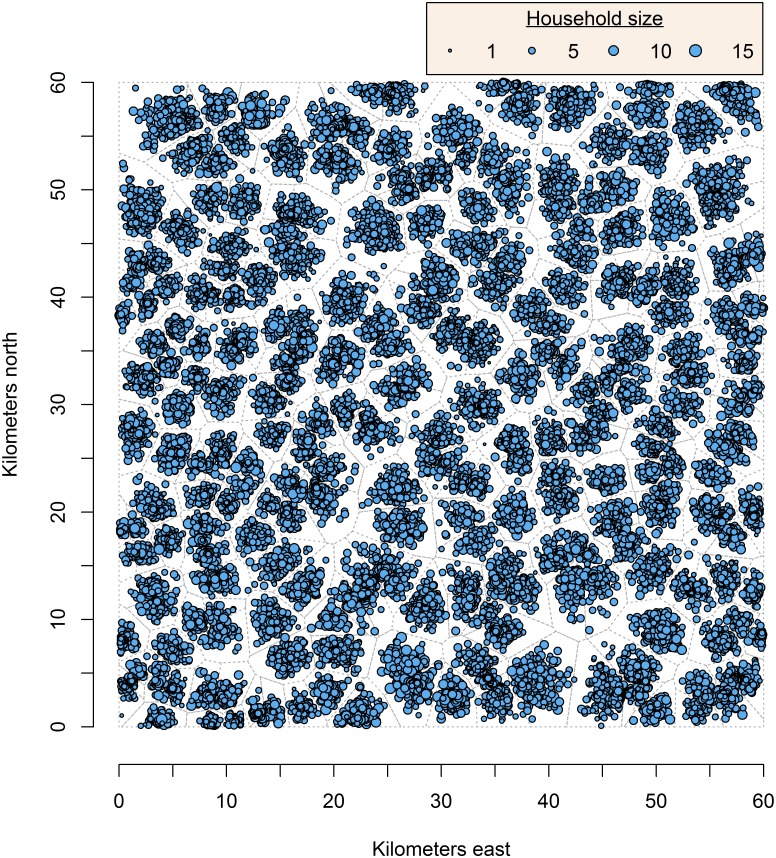
Methods: Five or ten microfoci of radius 1, 2, or 3 km with infection marker prevalence (intensity) of 3, 6, or 10 times background prevalence were placed in spatial simulations, run in R Version 3.2. Diagnostic tests included microfilaremia, immunochromatographic test (ICT), and Wb123 ELISA. Population size was fixed at 360,000 in a 60 x 60 km area; demographics were based on literature for Sub-Saharan African populations. Background ICT prevalence in 6-7 year olds was anchored at 1.0%, and the prevalence in the remaining population was adjusted by age. Adults≥18 years, women aged 15-40 years (WCBA), children aged 6-7 years, or children≤5 years were sampled. Cluster (CS), simple random sampling (SRS), and TAS-like sampling were simulated, with follow-up testing of the nearest 20, 100, or 500 persons around each infection-marker-positive person. A threshold number of positive persons in follow-up testing indicated a suspected microfocus. Suspected microfoci identified during surveillance and actual microfoci in the simulation were compared to obtain a predictive value positive (PVP). Each parameter set was referred to as a protocol. Protocols were scored by efficiency, defined as the most microfoci identified, the fewest persons requiring primary and follow-up testing, and the highest PVP. Negative binomial regression was used to estimate aggregate effects of different variables on efficiency metrics.
Results: All variables were significantly associated with efficiency metrics. Additional follow-up tests beyond 20 did not greatly increase the number of microfoci detected, but significantly negatively impacted efficiency. Of 3,402 protocols evaluated, 384 (11.3%) identified all five microfoci (PVP 3.4-100.0%) and required testing 0.73-35.6% of the population. All used SRS and 378 (98.4%) only identified all five microfoci if they were 2-3 km diameter or high-intensity (6x or 10x); 374 (97.4%) required ICT or Wb123 testing to identify all five microfoci, and 281 (73.0%) required sampling adults or WCBA. The most efficient CS protocols identified two (40%) microfoci. After limiting to protocols with 1-km radius microfoci of 3x intensity (n = 378), eight identified all five microfoci; all used SRS and ICT and required testing 31.2-33.3% of the population. The most efficient CS and TAS-like protocols as well as those using microfilaremia testing identified only one (20%) microfocus when they were limited to 1-km radius and 3x intensity.
Conclusion: In this model, SRS, ICT, and sampling of adults maximized microfocus detection efficiency. Follow-up sampling of more persons did not necessarily increase protocol efficiency. Current approaches towards surveillance, including TAS, may not detect small, low-intensity LF microfoci that could remain after cessation of MDA. The model provides many surveillance protocols that can be selected for optimal outcomes.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
A systematic review of alternative surveillance approaches for lymphatic filariasis in low prevalence settings: Implications for post-validation settings.PLoS Negl Trop Dis. 2020 May 12;14(5):e0008289. doi: 10.1371/journal.pntd.0008289. eCollection 2020 May. PLoS Negl Trop Dis. 2020. PMID: 32396575 Free PMC article.
-
Brugia Rapid™ antibody responses in communities of Indonesia in relation to the results of 'transmission assessment surveys' (TAS) for the lymphatic filariasis elimination program.Parasit Vectors. 2015 Oct 1;8:499. doi: 10.1186/s13071-015-1093-x. Parasit Vectors. 2015. PMID: 26427536 Free PMC article.
-
Potential strategies for strengthening surveillance of lymphatic filariasis in American Samoa after mass drug administration: Reducing 'number needed to test' by targeting older age groups, hotspots, and household members of infected persons.PLoS Negl Trop Dis. 2020 Dec 28;14(12):e0008916. doi: 10.1371/journal.pntd.0008916. eCollection 2020 Dec. PLoS Negl Trop Dis. 2020. PMID: 33370264 Free PMC article.
-
First evidence of lymphatic filariasis transmission interruption in Cameroon: Progress towards elimination.PLoS Negl Trop Dis. 2017 Jun 29;11(6):e0005633. doi: 10.1371/journal.pntd.0005633. eCollection 2017 Jun. PLoS Negl Trop Dis. 2017. PMID: 28662054 Free PMC article.
-
Assessment of transmission in areas of uncertain endemicity for lymphatic filariasis in Brazil.PLoS Negl Trop Dis. 2019 Nov 25;13(11):e0007836. doi: 10.1371/journal.pntd.0007836. eCollection 2019 Nov. PLoS Negl Trop Dis. 2019. PMID: 31765388 Free PMC article.
Cited by
-
Evaluation of lymphatic filariasis in endemic area of Brazil where mass drug administration is not required.Pathog Glob Health. 2019 May;113(3):143-148. doi: 10.1080/20477724.2019.1623546. Epub 2019 May 29. Pathog Glob Health. 2019. PMID: 31138026 Free PMC article.
-
General contextual effects on neglected tropical disease risk in rural Kenya.PLoS Negl Trop Dis. 2018 Dec 21;12(12):e0007016. doi: 10.1371/journal.pntd.0007016. eCollection 2018 Dec. PLoS Negl Trop Dis. 2018. PMID: 30576335 Free PMC article.
-
Reactive case detection can improve the efficiency of lymphatic filariasis surveillance compared to random sampling, Samoa 2023.PLoS Negl Trop Dis. 2025 Jul 11;19(7):e0012622. doi: 10.1371/journal.pntd.0012622. eCollection 2025 Jul. PLoS Negl Trop Dis. 2025. PMID: 40644410 Free PMC article.
-
The roadmap towards elimination of lymphatic filariasis by 2030: insights from quantitative and mathematical modelling.Gates Open Res. 2019 Sep 13;3:1538. doi: 10.12688/gatesopenres.13065.1. eCollection 2019. Gates Open Res. 2019. PMID: 31728440 Free PMC article.
-
Reassessment of areas with persistent Lymphatic Filariasis nine years after cessation of mass drug administration in Sri Lanka.PLoS Negl Trop Dis. 2017 Oct 30;11(10):e0006066. doi: 10.1371/journal.pntd.0006066. eCollection 2017 Oct. PLoS Negl Trop Dis. 2017. PMID: 29084213 Free PMC article.
References
-
- Klepac P, Metcalf CJ, McLean AR, Hampson K. Towards the endgame and beyond: complexities and challenges for the elimination of infectious diseases. Philosophical transactions of the Royal Society of London Series B, Biological sciences. 2013;368(1623):20120137 10.1098/rstb.2012.0137 ; - DOI - PMC - PubMed
-
- Henderson DA. Lessons from the eradication campaigns. Vaccine. 1999;17 Suppl 3:S53–5. . - PubMed
-
- World Health Organization. Planning for the Global Elimination of Trachoma (GET)1996. http://www.who.int/pbd/publications/trachoma/en/get_1996.pdf?ua=1.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
