

Clinical impact of chronic obstructive pulmonary disease on non-cystic fibrosis bronchiectasis. A study on 1,790 patients from the Spanish Bronchiectasis Historical Registry
- PMID: 28542286
- PMCID: PMC5436841
- DOI: 10.1371/journal.pone.0177931
Clinical impact of chronic obstructive pulmonary disease on non-cystic fibrosis bronchiectasis. A study on 1,790 patients from the Spanish Bronchiectasis Historical Registry
Abstract
Background: Few studies have evaluated the coexistence of bronchiectasis (BE) and chronic obstructive pulmonary disease (COPD) in series of patients diagnosed primarily with BE. The aim of this study was to analyse the characteristics of patients with BE associated with COPD included in the Spanish Bronchiectasis Historical Registry and compare them to the remaining patients with non-cystic fibrosis BE.
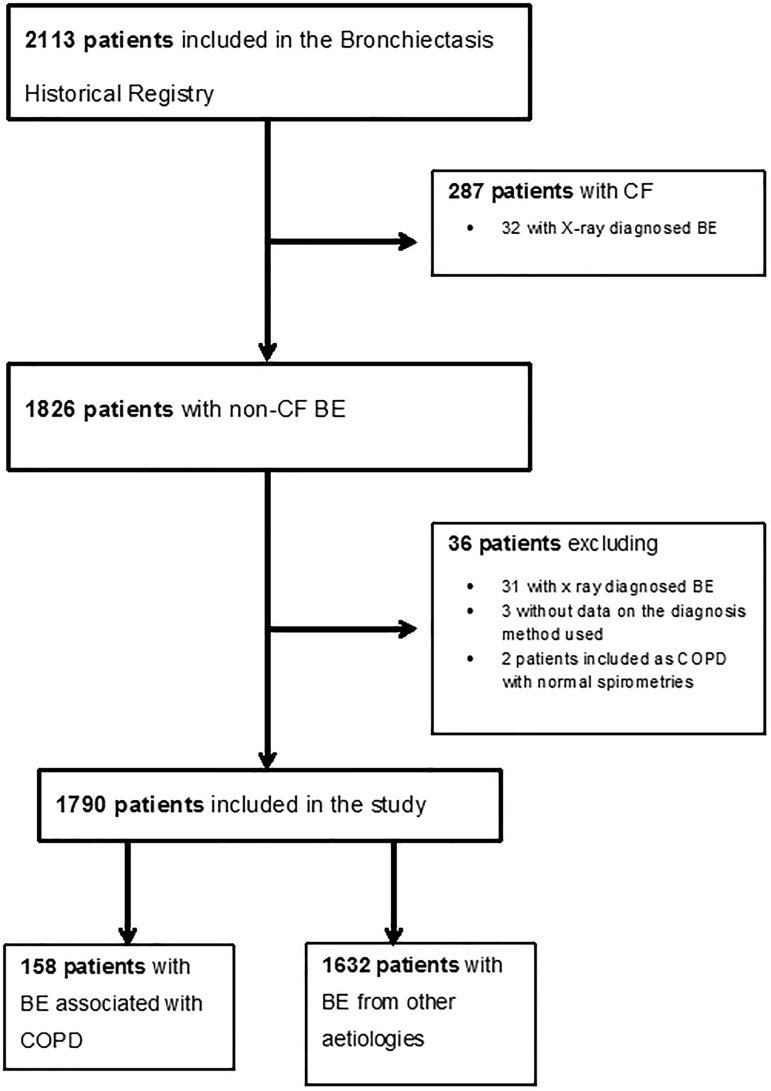
Methods: We conducted a multicentre observational study of historical cohorts, analysing the characteristics of 1,790 patients who had been included in the registry between 2002 and 2011. Of these, 158 (8.8%) were registered as BE related to COPD and were compared to the remaining patients with BE of other aetiologies.
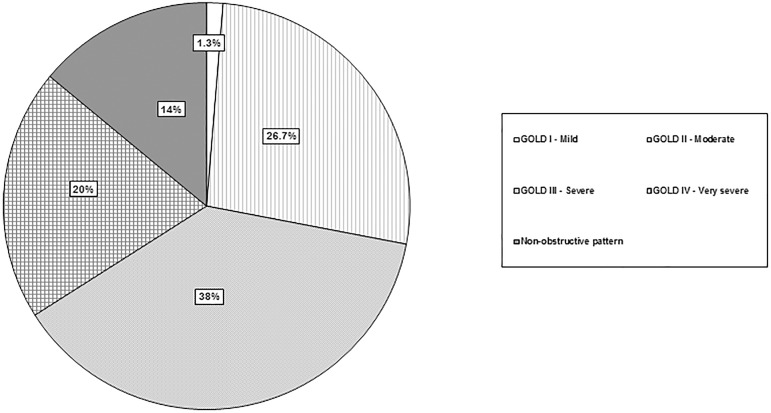
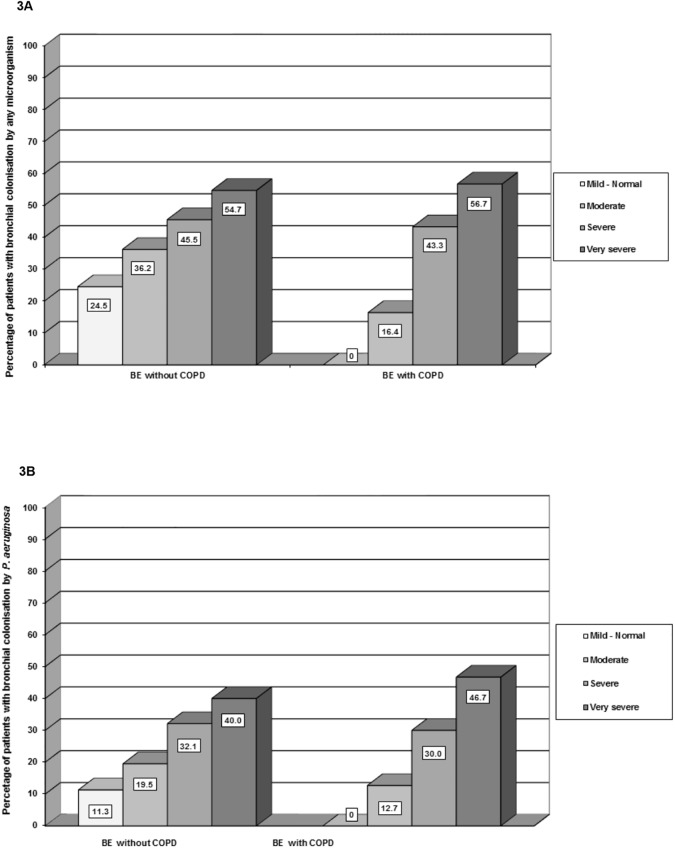
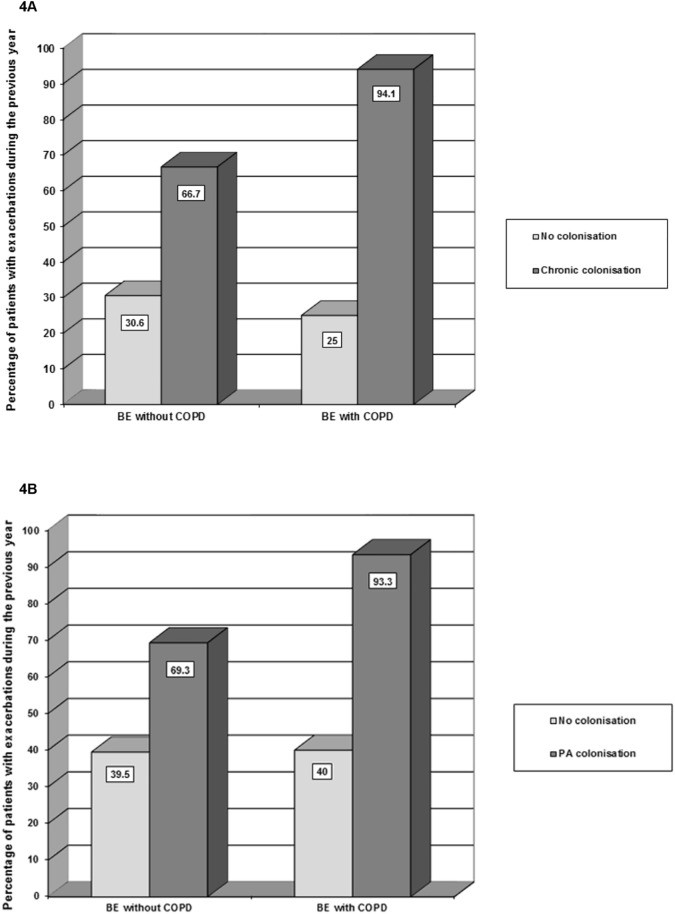
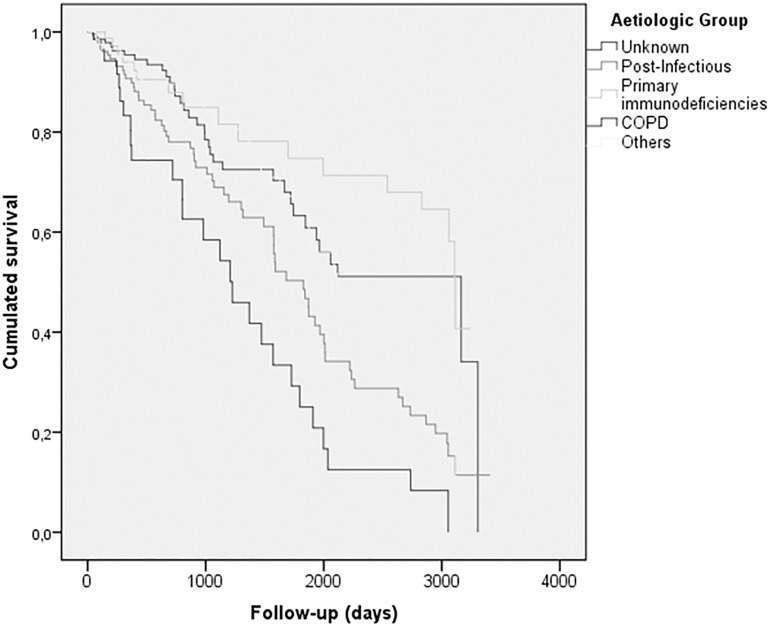
Results: Patients with COPD were mostly male, older, had a poorer respiratory function and more frequent exacerbations. There were no differences in the proportion of patients with chronic bronchial colonisation or in the isolated microorganisms. A significantly larger proportion of patients with COPD received treatment with bronchodilators, inhaled steroids and intravenous antibiotics, but there was no difference in the use of long term oral or inhaled antibiotherapy. During a follow-up period of 3.36 years, the overall proportion of deaths was 13.8%. When compared to the remaining aetiologies, patients with BE associated with COPD presented the highest mortality rate. The multivariate analysis showed that the diagnosis of COPD in a patient with BE as a primary diagnosis increased the risk of death by 1.77.
Conclusion: Patients with BE related to COPD have the same microbiological characteristics as patients with BE due to other aetiologies. They receive treatment with long term oral and inhaled antibiotics aimed at controlling chronic bronchial colonisation, even though the current COPD treatment guidelines do not envisage this type of therapy. These patients' mortality is notably higher than that of remaining patients with non-cystic fibrosis BE.
Conflict of interest statement
Figures
Similar articles
-
Etiology of Bronchiectasis in a Cohort of 2047 Patients. An Analysis of the Spanish Historical Bronchiectasis Registry.Arch Bronconeumol. 2017 Jul;53(7):366-374. doi: 10.1016/j.arbres.2016.12.003. Epub 2017 Jan 21. Arch Bronconeumol. 2017. PMID: 28118936 English, Spanish.
-
Noninvasive ventilation in chronic obstructive pulmonary disease, bronchiectasis and cystic fibrosis.Eur Respir J. 2002 Sep;20(3):777-84. doi: 10.1183/09031936.02.00308502. Eur Respir J. 2002. PMID: 12358358 Review.
-
The Association between Bronchiectasis and Chronic Obstructive Pulmonary Disease: Data from the European Bronchiectasis Registry (EMBARC).Am J Respir Crit Care Med. 2024 Jul 1;210(1):119-127. doi: 10.1164/rccm.202309-1614OC. Am J Respir Crit Care Med. 2024. PMID: 38271696
-
Bronchiectasis in Türkiye: Data from a Multicenter Registry (Turkish Adult Bronchiectasis Database).Balkan Med J. 2024 May 3;41(3):206-212. doi: 10.4274/balkanmedj.galenos.2024.2023-12-57. Balkan Med J. 2024. PMID: 38700365 Free PMC article.
-
Chronic obstructive pulmonary disease and bronchiectasis.Curr Opin Pulm Med. 2013 Mar;19(2):133-9. doi: 10.1097/MCP.0b013e32835d8312. Curr Opin Pulm Med. 2013. PMID: 23287285 Review.
Cited by
-
Association between Inhaled Corticosteroid Use and Pulmonary Nontuberculous Mycobacterial Infection.Ann Am Thorac Soc. 2018 Oct;15(10):1169-1176. doi: 10.1513/AnnalsATS.201804-245OC. Ann Am Thorac Soc. 2018. PMID: 30213194 Free PMC article.
-
Suspected Bronchiectasis and Mortality in Adults With a History of Smoking Who Have Normal and Impaired Lung Function : A Cohort Study.Ann Intern Med. 2023 Oct;176(10):1340-1348. doi: 10.7326/M23-1125. Epub 2023 Oct 3. Ann Intern Med. 2023. PMID: 37782931 Free PMC article.
-
ROSE: radiology, obstruction, symptoms and exposure - a Delphi consensus definition of the association of COPD and bronchiectasis by the EMBARC Airways Working Group.ERJ Open Res. 2021 Nov 22;7(4):00399-2021. doi: 10.1183/23120541.00399-2021. eCollection 2021 Oct. ERJ Open Res. 2021. PMID: 34820447 Free PMC article.
-
Chronic Obstructive Pulmonary Disease as a Phenotype of Bronchiectasis for Long-Term Clinical Presentation and Treatment.Medicina (Kaunas). 2021 Jun 5;57(6):579. doi: 10.3390/medicina57060579. Medicina (Kaunas). 2021. PMID: 34198847 Free PMC article.
-
Small Airway Disease and Emphysema Are Associated with Future Exacerbations in Smokers with CT-derived Bronchiectasis and COPD: Results from the COPDGene Cohort.Radiology. 2021 Sep;300(3):706-714. doi: 10.1148/radiol.2021204052. Epub 2021 Jun 22. Radiology. 2021. PMID: 34156303 Free PMC article.
References
-
- Barker AF, Bardana EJ. Bronchiectasis: update of an orphan disease. Am Rev Respir Dis 1988; 137: 969–78 doi: 10.1164/ajrccm/137.4.969 - DOI - PubMed
-
- Gao YH, Guan WJ, Liu SX, Wang L, Cui JJ, Chen RC, et al. Aetiology of bronchiectasis in adults: A systematic literature review. Respirology. 2016. June 19. - PubMed
-
- Du Q, Jin J, Liu X, Sun Y. Bronchiectasis as a Comorbidity of Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis. PLoS One. 2016. March 15;11(3):e0150532 doi: 10.1371/journal.pone.0150532 - DOI - PMC - PubMed
-
- Garcia-Vidal C, Almagro P, Romani V, Rodríguez-Carballeira M, Cuchi E, Canales L, et al. Pseudomonas aeruginosa in patients hospitalized for COPD exacerbation: a prospective study. Eur Respir J. 2009; 34: 1072–8. doi: 10.1183/09031936.00003309 - DOI - PubMed
-
- Gatheral T, Kumar N, Sansom B, Lai D, Nair A, Vlahos I, et al. COPD related bronchiectasis; independent impact on disease course and outcomes. COPD. 2014; 11:605–14. doi: 10.3109/15412555.2014.922174 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
