

Predictors of loss to follow-up among patients on ART at a rural hospital in KwaZulu-Natal, South Africa
- PMID: 28542309
- PMCID: PMC5443492
- DOI: 10.1371/journal.pone.0177168
Predictors of loss to follow-up among patients on ART at a rural hospital in KwaZulu-Natal, South Africa
Abstract
Introduction: Improved HIV outcomes as a result of expanded antiretroviral therapy (ART) access is threatened by increasing rates of loss to follow up (LTFU) among those on ART, largely reported in urban populations. Some reports suggest that LTFU rates are overestimated due to patient movement to other facilities and inadequate medical records.
Study objective: To define the proportion disengaging from HIV care as well as the characteristics of those LTFU in order to design and implement appropriate interventions to increase retention.
Methods: We performed a retrospective review of patients who discontinued ART at a central hospital ART clinic in rural South Africa and compared with patients receiving care at the 15 primary health clinics (PHCs) to determine the true proportion of those who were LTFU. We also compared those who discontinued ART with those who did not at the central hospital ART clinic to determine predictors of loss to follow up.
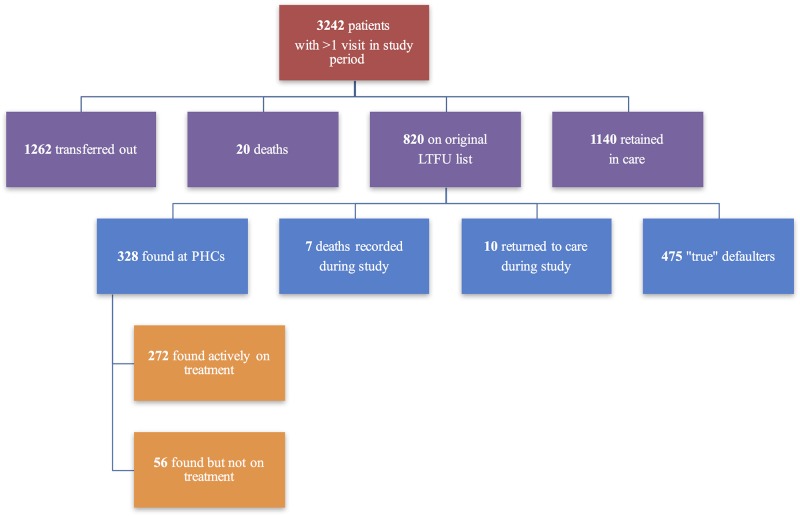
Results: Among 3242 patients on ART, 820 were originally marked as LTFU. Among all patients, 272 (8.4%) were found at a clinic on treatment, 56 (1.7%) were found at a clinic from which they had since discontinued treatment, and 10 (0.3%) returned to care between June and July 2016, leaving 475 (14.7%) unaccounted for and thus categorized as 'true' LTFU. Factors found to be associated with discontinuation include being male, age 18-35, having a CD4 count under 200 cells/μL, and being on ART for under six months.
Conclusions: Young men with low CD4 counts early after ART initiation are at highest risk of ART disengagement in this rural South African HIV clinic. Novel interventions targeting this group are needed to improve retention in care.
Conflict of interest statement
Figures
References
-
- WHO. Global health sector response to HIV, 200–2015: Focus on innovations in Africa: Progress report. World Health Organization, 2015.
-
- Shisana O, Rehle T, Simbayi LC, Zuma K, Jooste S, Zungu N, et al. South African National HIV Prevalence, Incidence and Behaviour Survey, 2012. Cape Town: HSRC Press; 2014. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
