

Patterns of Treatment Failure and Postrecurrence Outcomes Among Patients With Locally Advanced Head and Neck Squamous Cell Carcinoma After Chemoradiotherapy Using Modern Radiation Techniques
- PMID: 28542679
- PMCID: PMC5710194
- DOI: 10.1001/jamaoncol.2017.0973
Patterns of Treatment Failure and Postrecurrence Outcomes Among Patients With Locally Advanced Head and Neck Squamous Cell Carcinoma After Chemoradiotherapy Using Modern Radiation Techniques
Abstract
Importance: Even though 15% to 50% of patients with head and neck squamous cell carcinoma (HNSCC) experience recurrence, relatively little is known regarding patterns of treatment failure and postrecurrence outcomes after chemoradiotherapy using modern radiation techniques (intensity-modulated radiotherapy [IMRT]). Recurrence patterns are significantly affected by variations in the quality of radiotherapy, which may confound findings from multicenter trials.
Objective: To assess patterns of treatment failure and postrecurrence outcomes for patients with HNSCC treated with contemporary radiotherapy techniques.
Design, setting, and participants: This large single-institution cohort study reviewed the outcomes of 1000 consecutive patients with stage III to IVB oropharyngeal carcinoma (n = 703), laryngeal carcinoma (n = 126), or hypopharyngeal carcinoma (n = 46) treated with definitive IMRT with or without concurrent chemotherapy, as well as patients with oral cavity carcinoma (n = 125) treated with postoperative IMRT with or without concurrent systemic therapy, from December 1, 2001, to December 31, 2013, with a median follow-up of 65.1 months among surviving patients. Data analysis was performed from January 31, 2016, to February 17, 2017.
Main outcomes and measures: Patterns of treatment failure and overall survival following locoregional failure or distant metastasis.
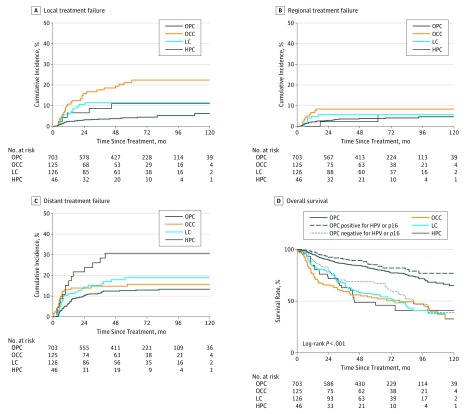
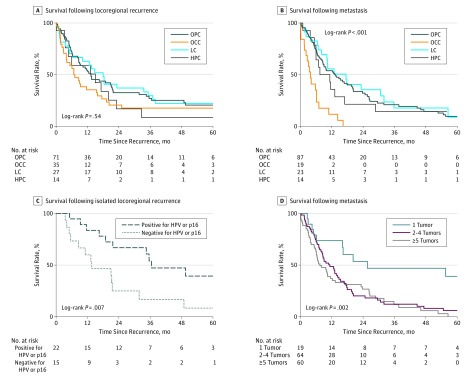
Results: Among the 1000 patients (186 women and 814 men; mean [SD] age, 59.3 [10.8] years), there were no marginal or isolated out-of-radiation-field failures. Among subsites, the cumulative incidence of local failure was highest among patients with oral cavity carcinoma vs those with oropharyngeal carcinoma (hazard ratio, 5.2; 95% CI, 3.1-8.6; P < .001). Furthermore, patients with oral cavity carcinoma experienced significantly shorter survival following distant metastasis (hazard ratio, 3.66; 95% CI, 1.98-6.80; P < .001). Patients with oropharyngeal carcinoma positive for human papillomavirus or p16 lived longer after locoregional failure compared with patents with oropharyngeal carcinoma negative for human papillomavirus or p16 (median survival, 36.5 vs 13.6 months; P = .007) but not after distant metastasis. Salvage surgery was associated with improved overall survival following locoregional failure (hazard ratio, 0.51; 95% CI, 0.34-0.77; P = .001); oligometastatic disease (1 vs ≥2 lesions: hazard ratio, 0.32; 95% CI, 0.16-0.63; P = .001) was associated with improved overall survival following distant metastasis.
Conclusions and relevance: Overall survival after recurrence of HNSCC is influenced by the HNSCC subsite and human papillomavirus or p16 status, as well surgical and systemic interventions. An oligometastatic phenotype characterizes patients with solitary metastasis after chemoradiotherapy. These findings have important implications for clinical trial designs for HNSCC in the recurrent and oligometastatic setting.
Conflict of interest statement
Figures
References
-
- Pfister DG. NCCN clinical practice guidelines in oncology: head and neck cancers. Version 1. https://www.nccn.org/professionals/physician_gls/pdf/head-and-neck.pdf. Accessed September 1, 2016.
-
- Chao KS, Ozyigit G, Tran BN, Cengiz M, Dempsey JF, Low DA. Patterns of failure in patients receiving definitive and postoperative IMRT for head-and-neck cancer. Int J Radiat Oncol Biol Phys. 2003;55(2):312-321. - PubMed
-
- Mendenhall WM, Amdur RJ, Morris CG, Kirwan JM, Li JG. Intensity-modulated radiotherapy for oropharyngeal squamous cell carcinoma. Laryngoscope. 2010;120(11):2218-2222. - PubMed
-
- Setton J, Caria N, Romanyshyn J, et al. Intensity-modulated radiotherapy in the treatment of oropharyngeal cancer: an update of the Memorial Sloan-Kettering Cancer Center experience. Int J Radiat Oncol Biol Phys. 2012;82(1):291-298. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
