

Recognition of early mortality in multiple myeloma by a prediction matrix
- PMID: 28543165
- PMCID: PMC5601204
- DOI: 10.1002/ajh.24796
Recognition of early mortality in multiple myeloma by a prediction matrix
Abstract
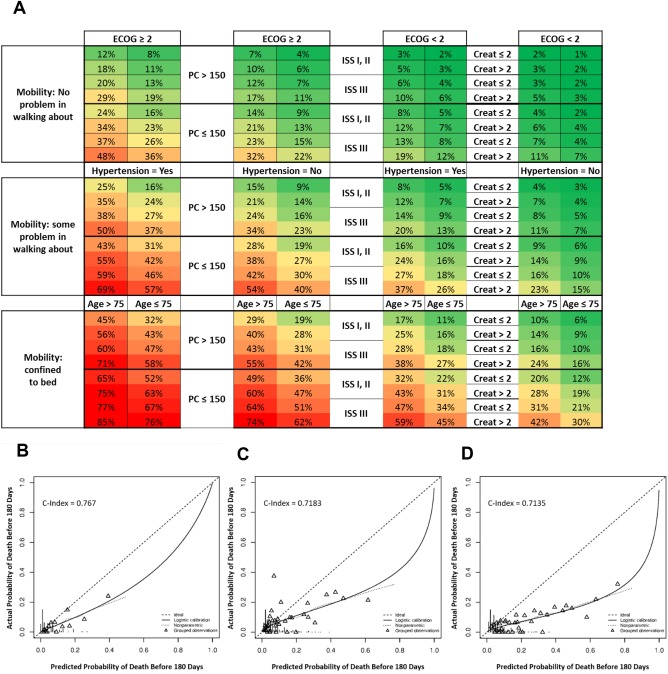
Early mortality (EM; death ≤ 6 months from diagnosis) has been reported in several newly diagnosed multiple myeloma (NDMM) trials. Before the era of novel agents, the incidence was 10%-14%. Causes of death included infections/pneumonia, renal failure, refractory disease, and cardiac events. Staging systems, such as the revised International Staging System (r-ISS), and prognostic factors including cytogenetics, lactate dehydrogenase levels, and myeloma-specific factors, are useful to assess overall prognosis; however, they cannot predict EM. We evaluated patients treated with novel agents in the Connect MM® Registry and identified risk factors of the EM cohort. Eligible patients were enrolled in the registry within 60 days of diagnosis. Univariate and multivariate analyses were conducted to evaluate associations between baseline characteristics and EM. Prediction matrices for EM were constructed from a logistic model. Between September 2009 and December 2011, 1493 patients were enrolled in the registry and had adequate follow-up. Of these patients, 102 (6.8%) had EM and 1391 (93.2%) survived for > 180 days. Baseline factors significantly associated with increased EM risk included age > 75 years, higher Eastern Cooperative Oncology Group performance status, lower EQ-5D mobility score, higher ISS stage, lower platelet count, and prior hypertension. Renal insufficiency trended toward increased EM risk. These risk factors were incorporated into a prediction matrix for EM. The EM prediction matrix uses differential weighting of risk factors to calculate EM risk in patients with NDMM. Identifying patients at risk for EM may provide new opportunities to implement patient-specific treatment strategies to improve outcomes.
© 2017 The Authors American Journal of Hematology Published by Wiley Periodicals, Inc.
Figures
References
-
- Murakami H, Hayashi K, Hatsumi N, et al. Risk factors for early death in patients undergoing treatment for multiple myeloma. Ann Hematol. 2001;80:452–455. - PubMed
-
- Kastritis E, Terpos E, Roussou M, et al. Very early death (< 2 months) in myeloma is associated with advanced age, poor performance status and reduced use of novel agents, while early death within 12 months is associated with high risk features of both the disease and the patient. Blood. 2013;122:[abstract 3195].
-
- Biran N, Jagannath S, Chari A. Risk stratification in multiple myeloma, part 1: characterization of high‐risk disease. Clin Adv Hematol Oncol. 2013;11:489–503. - PubMed
-
- Larocca A, Bringhen S, Petrucci M, et al. Early mortality in elderly newly diagnosed multiple myeloma patients treate with novel agents: a pooled analysis of two large randomized pahse III trials. Haematologica. 2015;100:[abstract P270]. - PubMed
-
- Augustson BM, Begum G, Dunn JA, et al. Early mortality after diagnosis of multiple myeloma: analysis of patients entered onto the United Kingdom Medical Research Council trials between 1980 and 2002–Medical Research Council Adult Leukaemia Working Party. J Clin Oncol. 2005;23:9219–9226. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical