

Undetectable Concentrations of a Food and Drug Administration-approved High-sensitivity Cardiac Troponin T Assay to Rule Out Acute Myocardial Infarction at Emergency Department Arrival
- PMID: 28544100
- PMCID: PMC5656889
- DOI: 10.1111/acem.13229
Undetectable Concentrations of a Food and Drug Administration-approved High-sensitivity Cardiac Troponin T Assay to Rule Out Acute Myocardial Infarction at Emergency Department Arrival
Abstract
Background: The objective of this study was to quantify the sensitivity of very low concentrations of high-sensitivity cardiac troponin T (hsTnT) at ED arrival for acute myocardial infarction (AMI) in a large cohort of chest pain patients evaluated in real-world clinical practice.
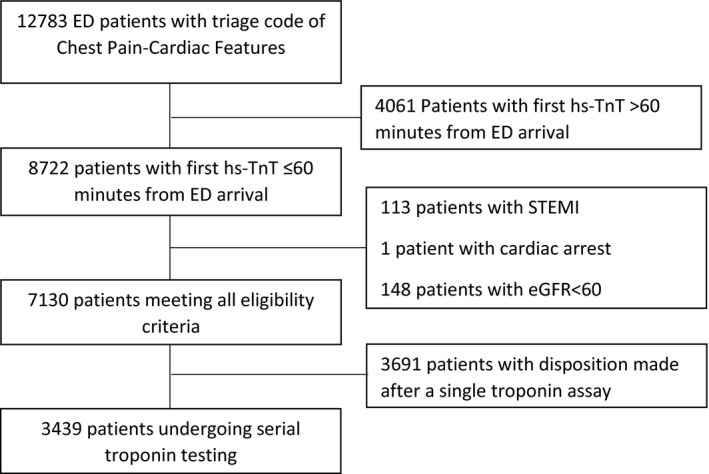
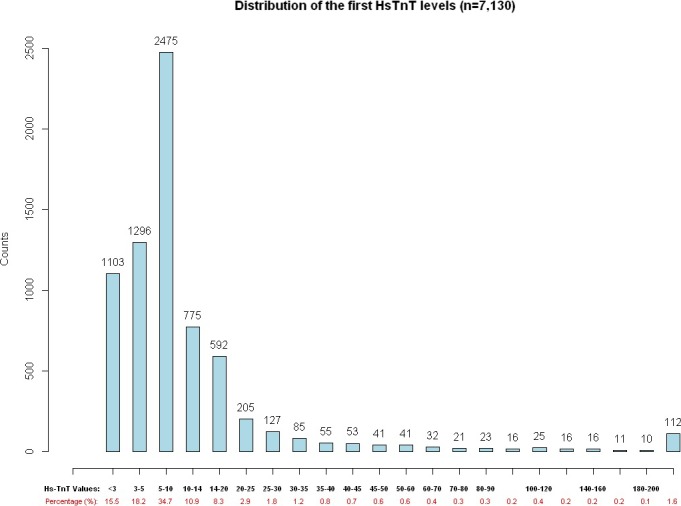
Methods: This retrospective study included consecutive ED patients with suspected cardiac chest pain evaluated in four urban EDs, excluding those with ST-elevation AMI, cardiac arrest or abnormal kidney function. The primary outcomes were AMI at 7, 30, and 90 days. Secondary outcomes included major adverse cardiac events (MACE; all-cause mortality, AMI, and revascularization) and the individual MACE components. Test characteristics were calculated for hsTnT values from 3 to 200 ng/L .
Results: A total of 7,130 patients met inclusion criteria. AMI incidences at 7, 30, and 90 days were 5.8, 6.0, and 6.2%. When the hsTnT assay was performed at ED arrival, the limit of blank of the assay (3 ng/L) ruled out 7-day AMI in 15.5% of patients with 100% sensitivity and negative predictive value (NPV). The limit of detection of the assay (5 ng/L) ruled out AMI in 33.6% of patients with 99.8% sensitivity and 99.95% NPV for 7-day AMI. The limit of quantification (the Food and Drug Administration [FDA]-approved cutoff for lower the reportable limit) of 6 ng/L ruled out AMI in 42.2% of patients with 99.8% sensitivity and 99.95% NPV. The sensitivities of the cutoffs of <3, <5, and <6 ng/L for 7-day MACE were 99.6, 97.4, and 96.6%, respectively. The NPVs of the cutoffs of <3, <5, and <6 ng/L for 7-day MACE were 99.8, 99.5, and 99.4%, respectively. A secondary analysis was performed in a subgroup of 3,549 higher-risk patients who underwent serial troponin testing. In this subgroup, a cutoff of 3 ng/L ruled out 7-day AMI in 9.6% of patients with 100% sensitivity and NPV, a cutoff of 5 ng/L ruled out 7-day AMI in 23.3% of patients with 99.7% sensitivity and 99.9% NPV, and a cutoff of 6 ng/L ruled out 7-day AMI in 29.8% of patients with 99.7 and 99.9% NPV. In the higher-risk subgroup, the sensitivities of cutoffs of <3, <5, and <6 ng/L for 7-day MACE were 99.8, 97.4, and 96.6%, respectively. In this higher-risk subgroup, the NPV of cutoffs of <3, <5, and <6 ng/L for 7-day MACE were 99.7, 98.5, and 98.4%, respectively.
Conclusions: When used in real-world clinical practice conditions, hsTnT concentrations < 6 ng/L (below the lower reportable limit for an FDA-approved assay) at the time of ED arrival can rule out AMI with very high sensitivity and NPV. The sensitivity for MACE is unacceptably low, and thus a single-troponin rule-out strategy should only be used in the context of a structured risk evaluation.
© 2017 The Authors. Academic Emergency Medicine published by Wiley Periodicals, Inc. on behalf of Society for Academic Emergency Medicine.
Figures
Comment in
-
Welcome to the Real World: Do the Conditions of FDA Approval Devalue High-sensitivity Troponin?Acad Emerg Med. 2017 Oct;24(10):1278-1280. doi: 10.1111/acem.13256. Epub 2017 Sep 18. Acad Emerg Med. 2017. PMID: 28715149 No abstract available.
References
-
- Buhuiya FA, Pitts SR, McCaig LF. Emergency department visits for chest pain and abdominal pain: United States, 1999–2008. NCHS Data Brief 2010;(43):1–8. - PubMed
-
- Than M, Herbert M, Flaws D, et al. What is an acceptable risk of major adverse cardiac event in chest pain patients soon after emergency department discharge from the emergency department? A clinical survey. Int J Cardiol 2013;166:752–4. - PubMed
-
- MacGougan CK, Christenson J, Innes G, Raboud J. Emergency physicians’ attitudes toward a clinical prediction rule for the identification and early discharge of low risk patients with chest discomfort. CJEM 2001;3:89–94. - PubMed
-
- Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 ACC/AHA Guideline for the management of patients with non‐ST‐elevation acute coronary syndromes. J Am Coll Cardiol 2014;64:e143–228. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
