

Presurgical language fMRI: Mapping of six critical regions
- PMID: 28544168
- PMCID: PMC5518223
- DOI: 10.1002/hbm.23661
Presurgical language fMRI: Mapping of six critical regions
Abstract
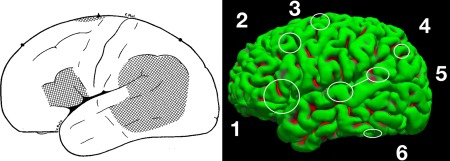
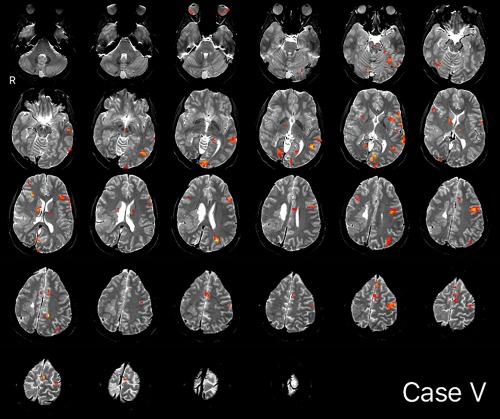
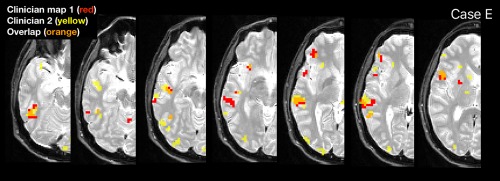
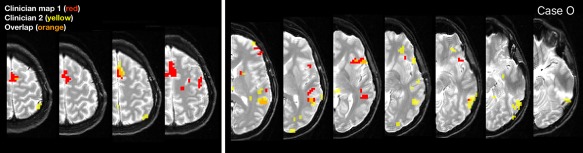
Language mapping is a key goal in neurosurgical planning. fMRI mapping typically proceeds with a focus on Broca's and Wernicke's areas, although multiple other language-critical areas are now well-known. We evaluated whether clinicians could use a novel approach, including clinician-driven individualized thresholding, to reliably identify six language regions, including Broca's Area, Wernicke's Area (inferior, superior), Exner's Area, Supplementary Speech Area, Angular Gyrus, and Basal Temporal Language Area. We studied 22 epilepsy and tumor patients who received Wada and fMRI (age 36.4[12.5]; Wada language left/right/mixed in 18/3/1). fMRI tasks (two × three tasks) were analyzed by two clinical neuropsychologists who flexibly thresholded and combined these to identify the six regions. The resulting maps were compared to fixed threshold maps. Clinicians generated maps that overlapped significantly, and were highly consistent, when at least one task came from the same set. Cases diverged when clinicians prioritized different language regions or addressed noise differently. Language laterality closely mirrored Wada data (85% accuracy). Activation consistent with all six language regions was consistently identified. In blind review, three external, independent clinicians rated the individualized fMRI language maps as superior to fixed threshold maps; identified the majority of regions significantly more frequently; and judged language laterality to mirror Wada lateralization more often. These data provide initial validation of a novel, clinician-based approach to localizing language cortex. They also demonstrate clinical fMRI is superior when analyzed by an experienced clinician and that when fMRI data is of low quality judgments of laterality are unreliable and should be withheld. Hum Brain Mapp 38:4239-4255, 2017. © 2017 Wiley Periodicals, Inc.
Keywords: epilepsy; fMRI; language; neurology; neuropsychology; surgery.
© 2017 The Authors Human Brain Mapping Published by Wiley Periodicals, Inc.
Figures

References
-
- American College of Radiology (2014): ACR–ASNR–SPR Practice Parameter for the Performance of Functional Magnetic Resonance Imaging (fMRI) of the Brain. Res 39.
-
- Anderson S, Damasio A, Damasio H (1990): Troubled letters but not numbers. Brain 113:749–766. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
