

CXCL10 and IL-6: Markers of two different forms of intra-amniotic inflammation in preterm labor
- PMID: 28544362
- PMCID: PMC5488235
- DOI: 10.1111/aji.12685
CXCL10 and IL-6: Markers of two different forms of intra-amniotic inflammation in preterm labor
Abstract
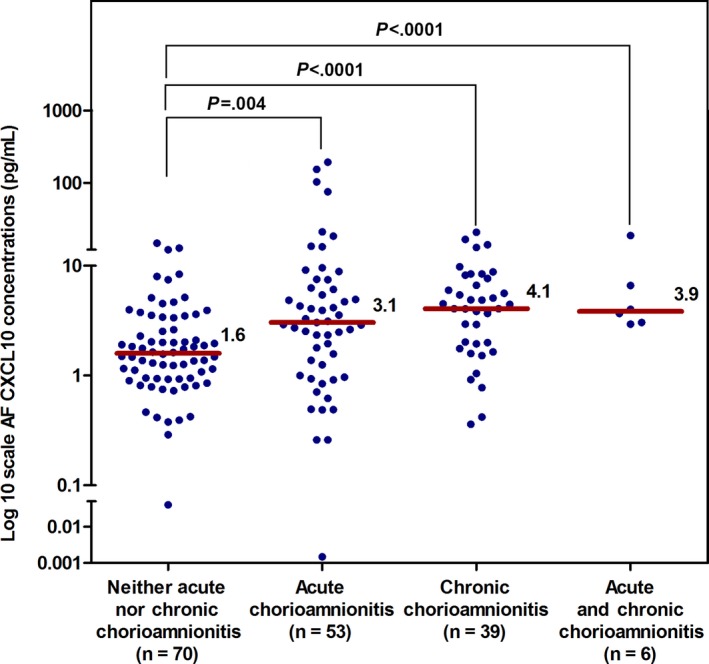
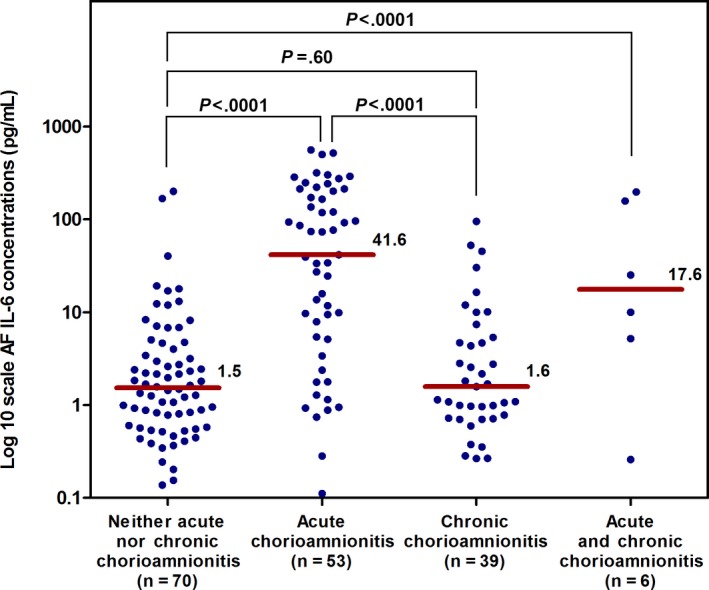
Problem: To determine whether amniotic fluid (AF) CXCL10 concentration is associated with histologic chronic chorioamnionitis in patients with preterm labor (PTL) and preterm prelabor rupture of the membranes (PROM).
Method of study: This study included 168 women who had an episode of PTL or preterm PROM. AF interleukin (IL)-6 and CXCL10 concentrations were determined by immunoassay.
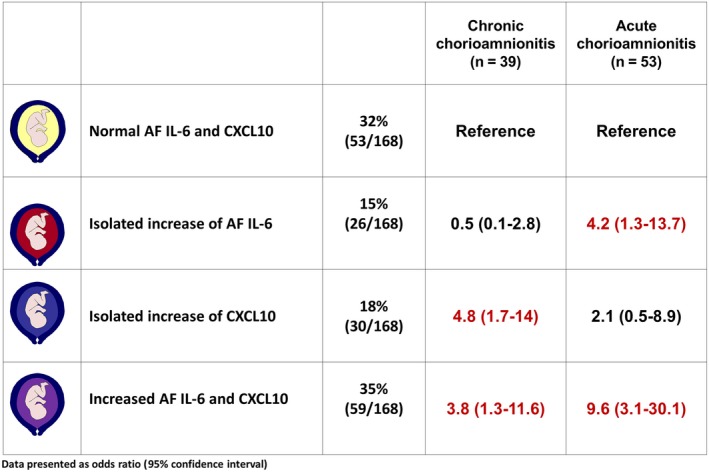
Results: (i) Increased AF CXCL10 concentration was associated with chronic (OR: 4.8; 95% CI: 1.7-14), but not acute chorioamnionitis; (ii) increased AF IL-6 concentration was associated with acute (OR: 4.2; 95% CI: 1.3-13.7) but not chronic chorioamnionitis; and (iii) an increase in AF CXCL10 concentration was associated with placental lesions consistent with maternal anti-fetal rejection (OR: 3.7; 95% CI: 1.3-10.4). (iv) All patients with elevated AF CXCL10 and IL-6 delivered preterm.
Conclusion: Increased AF CXCL10 concentration is associated with chronic chorioamnionitis or maternal anti-fetal rejection, whereas increased AF IL-6 concentration is associated with acute histologic chorioamnionitis.
Keywords: allograft; amniocentesis; biomarker; chorioamnionitis; chronic inflammation; cytokine; maternal anti-fetal rejection.
Published 2017. This article is a U.S. Government work and is in the public domain in the USA. American Journal of Reproductive Immunology published by John Wiley & Sons Ltd.
Figures

References
-
- Wilkins I, Creasy RK. Preterm labor. Clin Obstet Gynecol. 1990;33:502‐514. - PubMed
-
- Romero R, Mazor M, Munoz H, Gomez R, Galasso M, Sherer DM. The preterm labor syndrome. Ann N Y Acad Sci. 1994;734:414‐429. - PubMed
-
- Mazor M, Chaim W, Romero R. [Preterm labor syndrome]. Harefuah. 1995;128:111‐116. - PubMed
-
- Romero R, Gomez R, Mazor M, Ghezzi F, Yoon BH. The preterm labor syndrome In: Elder MG, Romero R, Lamont RF, eds. Preterm Labor. New York: Churchill Livingstone; 1997:29‐49.
-
- Dudley DJ. Pre‐term labor: an intra‐uterine inflammatory response syndrome? J Reprod Immunol. 1997;36:93‐109. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
