

Cluster-Randomized Trial of a Behavioral Intervention to Incorporate a Treat-to-Target Approach to Care of US Patients With Rheumatoid Arthritis
- PMID: 28544704
- PMCID: PMC5873265
- DOI: 10.1002/acr.23294
Cluster-Randomized Trial of a Behavioral Intervention to Incorporate a Treat-to-Target Approach to Care of US Patients With Rheumatoid Arthritis
Abstract
Objective: To assess the feasibility and efficacy of implementing a treat-to-target approach versus usual care in a US-based cohort of rheumatoid arthritis patients.
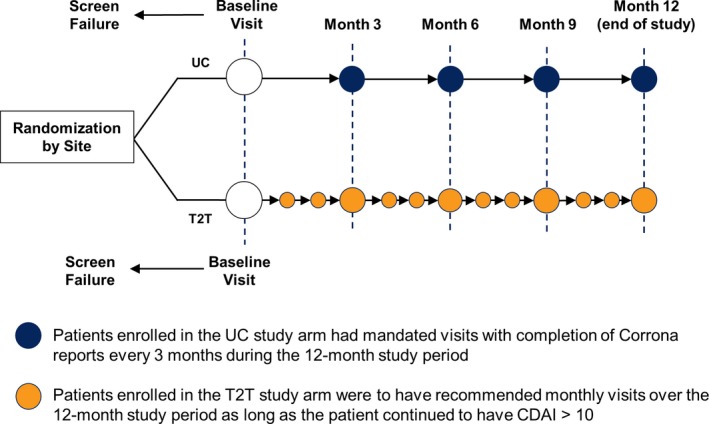
Methods: In this behavioral intervention trial, rheumatology practices were cluster-randomized to provide treat-to-target care or usual care. Eligible patients with moderate/high disease activity (Clinical Disease Activity Index [CDAI] score >10) were followed for 12 months. Both treat-to-target and usual care patients were seen every 3 months. Treat-to-target providers were to have monthly visits with treatment acceleration at a minimum of every 3 months in patients with CDAI score >10; additional visits and treatment acceleration were at the discretion of usual care providers and patients. Coprimary end points were feasibility, assessed by rate of treatment acceleration conditional on CDAI score >10, and achievement of low disease activity (LDA; CDAI score ≤10) by an intent-to-treat analysis.
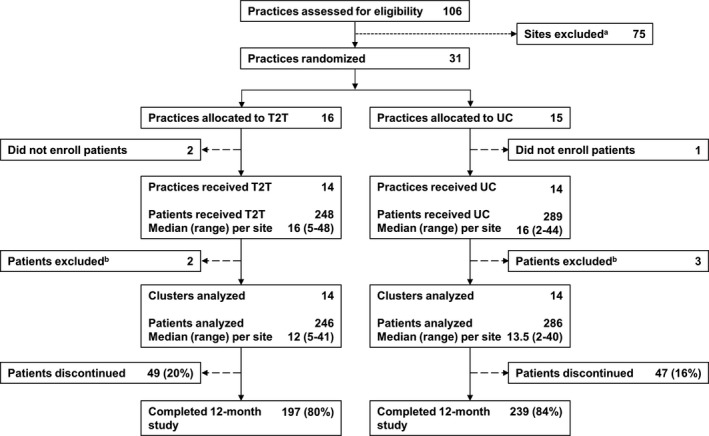
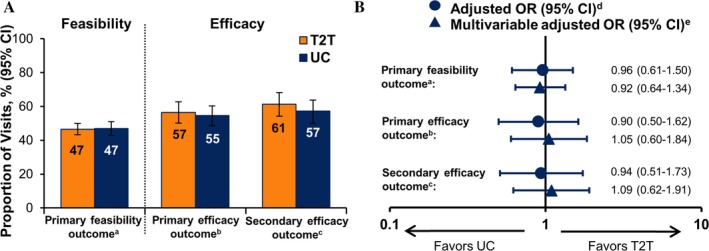
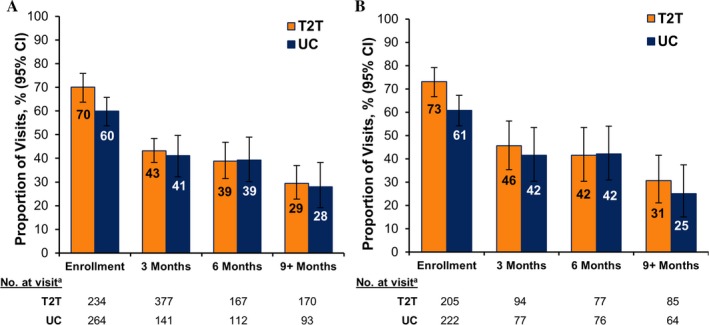
Results: A total of 14 practice sites per study arm were included (246 patients receiving treat-to-target and 286 receiving usual care). The groups had similar baseline demographic and clinical characteristics. Rates of treatment acceleration (treat-to-target 47% versus usual care 50%; odds ratio [OR] 0.92 [95% confidence interval (95% CI) 0.64, 1.34]) and achievement of LDA (treat-to-target 57% versus usual care 55%; OR 1.05 [95% CI 0.60, 1.84]) were similar between groups. Treat-to-target providers reported patient reluctance and medication lag time as common barriers to treatment acceleration.
Conclusion: This study is the first to examine the feasibility and efficacy of a treat-to-target approach in typical US rheumatology practice. Treat-to-target care was not associated with increased likelihood of treatment acceleration or achievement of LDA, and barriers to treatment acceleration were identified.
© 2017, The Authors. Arthritis Care & Research published by Wiley Periodicals, Inc. on behalf of American College of Rheumatology.
Figures
References
-
- Grigor C, Capell H, Stirling A, McMahon AD, Lock P, Vallance R, et al. Effect of a treatment strategy of tight control for rheumatoid arthritis (the TICORA study): a single‐blind randomised controlled trial. Lancet 2004;364:263–9. - PubMed
-
- Schipper LG, Vermeer M, Kuper HH, Hoekstra MO, Haagsma CJ, Den Broeder AA, et al. A tight control treatment strategy aiming for remission in early rheumatoid arthritis is more effective than usual care treatment in daily clinical practice: a study of two cohorts in the Dutch Rheumatoid Arthritis Monitoring registry. Ann Rheum Dis 2012;71:845–50. - PubMed
-
- Verstappen SM, Jacobs JW, van der Veen MJ, Heurkens AH, Schenk Y, ter Borg EJ, et al. Intensive treatment with methotrexate in early rheumatoid arthritis: aiming for remission. Computer Assisted Management in Early Rheumatoid Arthritis (CAMERA, an open‐label strategy trial). Ann Rheum Dis 2007;66:1443–9. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
