

Direct and indirect costs of diabetes mellitus in Mali: A case-control study
- PMID: 28545129
- PMCID: PMC5436679
- DOI: 10.1371/journal.pone.0176128
Direct and indirect costs of diabetes mellitus in Mali: A case-control study
Abstract
Background: Diabetes mellitus (DM) is one of the most burdensome chronic diseases and is associated with shorter lifetime, diminished quality of life and economic burdens on the patient and society as a result of healthcare, medication, and reduced labor market participation. We aimed to estimate the direct (medical and non-medical) and indirect costs of DM and compare them with those of people without DM (ND), as well as the cost predictors.
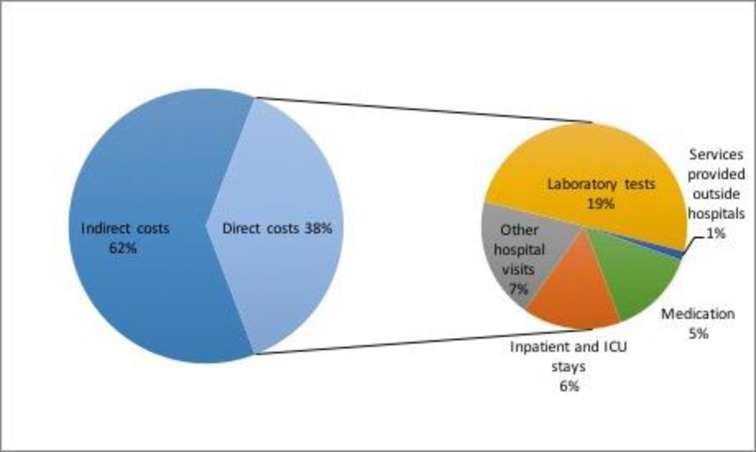
Methods and findings: Observational retrospective case-control study performed in Mali. Participants were identified and randomly selected from diabetes registries. We recruited 500 subjects with DM and 500 subjects without DM, matched by sex and age. We conducted structured, personal interviews. Costs were expressed for a 90-day period. Direct medical costs comprised: inpatient stays, ICU, laboratory tests and other hospital visits, specialist and primary care doctor visits, others, traditional practitioners, and medication. Direct non-medical costs comprised travel for treatment and paid caregivers. The indirect costs include the productivity losses by patients and caregivers, and absenteeism. We estimate a two-part model by type of service and a linear multiple regression model for the total cost. We found that total costs of persons with DM were almost 4 times higher than total cost of people without DM. Total costs were $77.08 and $281.92 for ND and DM, respectively, with a difference of $204.84.
Conclusions: Healthcare use and costs were dramatically higher for people with DM than for people with normal glucose tolerance and, in relative terms, much higher than in developed countries.
Conflict of interest statement
Figures

References
-
- Institute for Health Metrics and Evaluation, Human Development Network, The World Bank. The Global Burden of Disease: Generating Evidence, Guiding Policy—Sub-Saharan Africa Regional Edition. Seattle, WA: IHME, 2013.
-
- Jaffiol C. [The burden of diabetes in Africa: a major public health problem]. Bull Acad Natl Med. 2011. June;195(6):1239–53; discussion 1253–4. - PubMed
-
- International Diabetes Federation. IDF Diabetes Atlas, 7th edn Brussels, Belgium: International Diabetes Federation, 2015. http://www.idf.org/diabetesatlas.
-
- Mohan V, Madan Z, Jha R, Deepa R, Pradeepa R. Diabetes-social and economic perspectives in the new millennium. International journal of diabetes in developing countries 2004, 24:29–35.
-
- World Health Organization. Designing health financing systems to reduce catastrophic health expenditure. Technical briefs for policy makers number 2. (WHO/EIP/HSF/PB/05.02) Geneva: WHO; 2005.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
