

Diagnostic performance of serum blood urea nitrogen to creatinine ratio for distinguishing prerenal from intrinsic acute kidney injury in the emergency department
- PMID: 28545421
- PMCID: PMC5445342
- DOI: 10.1186/s12882-017-0591-9
Diagnostic performance of serum blood urea nitrogen to creatinine ratio for distinguishing prerenal from intrinsic acute kidney injury in the emergency department
Abstract
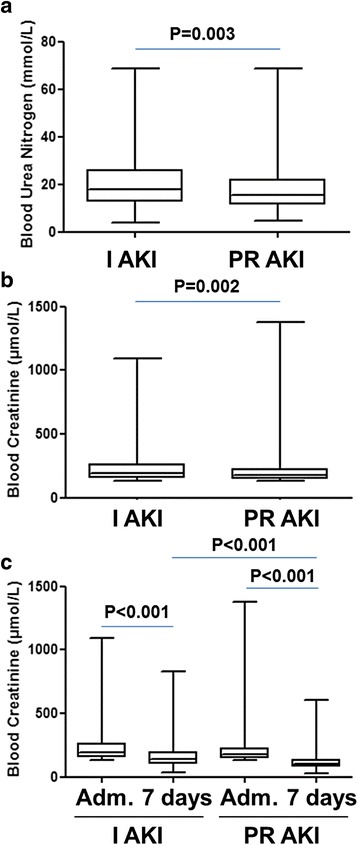
Background: The blood urea nitrogen to creatinine ratio (BCR) has been used since the early 1940s to help clinicians differentiate between prerenal acute kidney injury (PR AKI) and intrinsic AKI (I AKI). This ratio is simple to use and often put forward as a reliable diagnostic tool even though little scientific evidence supports this. The aim of this study was to determine whether BCR is a reliable tool for distinguishing PR AKI from I AKI.
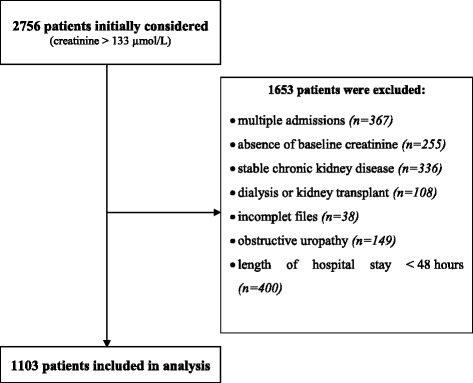
Methods: We conducted a retrospective observational study over a 13 months period, in the Emergency Department (ED) of Nantes University Hospital. Eligible for inclusion were all adult patients consecutively admitted to the ED with a creatinine >133 μmol/L (1.5 mg/dL).
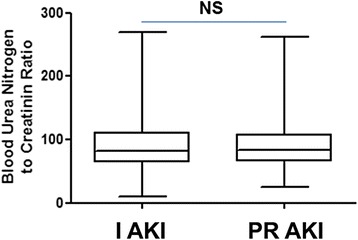
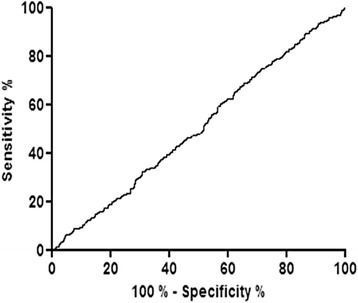
Results: Sixty thousand one hundred sixty patients were consecutively admitted to the ED. 2756 patients had plasma creatinine levels in excess of 133 μmol/L, 1653 were excluded, leaving 1103 patients for definitive inclusion. Mean age was 75.7 ± 14.8 years old, 498 (45%) patients had PR AKI and 605 (55%) I AKI. BCR was 90.55 ± 39.32 and 91.29 ± 39.79 in PR AKI and I AKI groups respectively. There was no statistical difference between mean BCR of the PR AKI and I AKI groups, p = 0.758. The area under the ROC curve was 0.5 indicating that BCR had no capacity to discriminate between PR AKI and I AKI.
Conclusions: Our study is the largest to investigate the diagnostic performance of BCR. BCR is not a reliable parameter for distinguishing prerenal AKI from intrinsic AKI.
Keywords: Acute kidney injury (AKI); Blood urea creatinine ratio (BCR); Diagnostic performance; Emergency department; Prerenal acute kidney injury.
Figures
References
-
- Fishberg AM. Hypertension and nephritis, in Lea & Febiger (eds): Philadelphia, 1939.
-
- Lin J, Denker BM. Azotemia and urinary abnormalities. In: Kasper DL, editor. Harrison’s principles of internal medicine. 19th. New York: McGraw Hill Education; 2015. pp. 289–295.
-
- Wolfson AB. Renal failure. In: Marx JA, Rosen P, editors. Rosen’s emergency medicine: concepts and clinical practice. 8th. Philadelphia: Elsevier/Saunders; 2014. pp. 1291–1311.
-
- Steddon S, Chesser A, Cunningham J, Ashman N. Acute kidney injury; in Singh P, Fenech LE (eds): Oxford Handbook of Nephrology and Hypertension, 2nd ed. New York: Oxford University Press, 2014; pp87–189.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
