

Seattle Heart Failure and Proportional Risk Models Predict Benefit From Implantable Cardioverter-Defibrillators
- PMID: 28545633
- PMCID: PMC5502749
- DOI: 10.1016/j.jacc.2017.03.568
Seattle Heart Failure and Proportional Risk Models Predict Benefit From Implantable Cardioverter-Defibrillators
Abstract
Background: Recent clinical trials highlight the need for better models to identify patients at higher risk of sudden death.
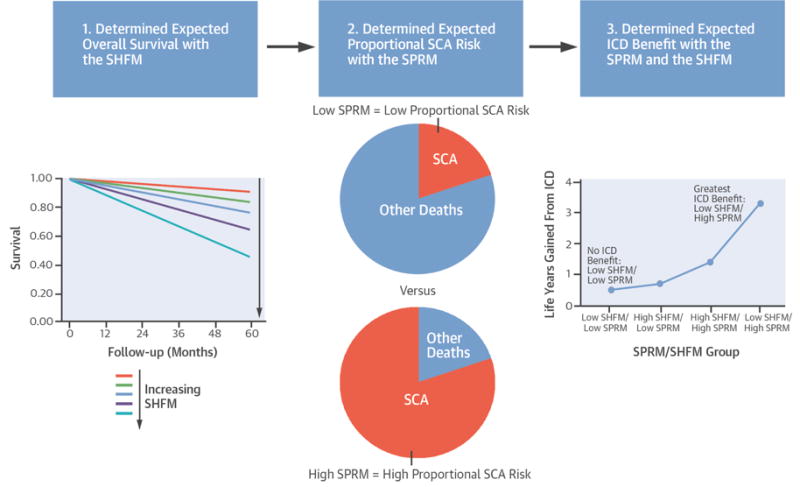
Objectives: The authors hypothesized that the Seattle Heart Failure Model (SHFM) for overall survival and the Seattle Proportional Risk Model (SPRM) for proportional risk of sudden death, including death from ventricular arrhythmias, would predict the survival benefit with an implantable cardioverter-defibrillator (ICD).
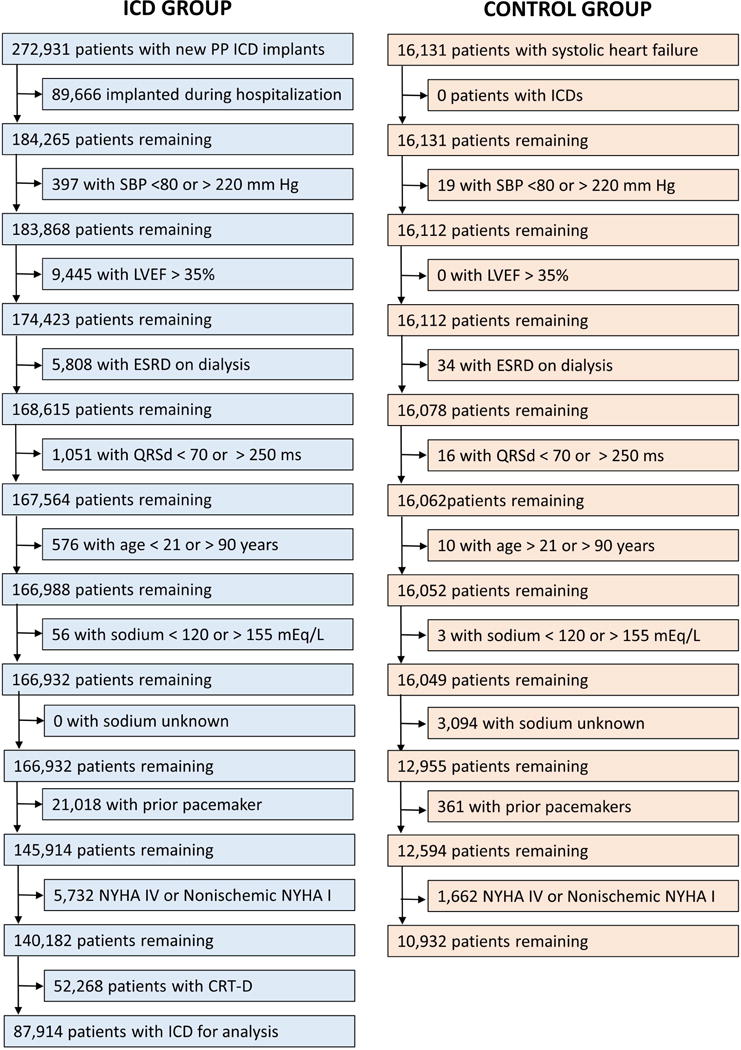
Methods: Patients with primary prevention ICDs from the National Cardiovascular Data Registry (NCDR) were compared with control patients with heart failure (HF) without ICDs with respect to 5-year survival using multivariable Cox proportional hazards regression.
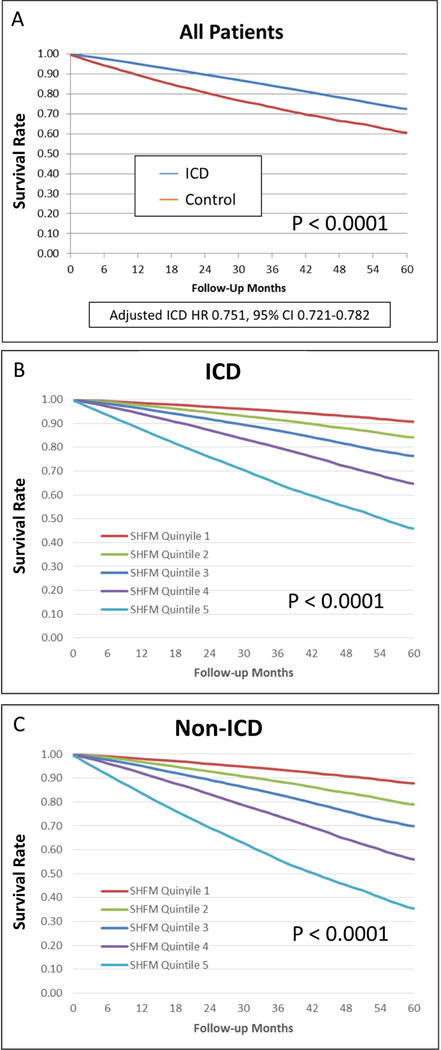
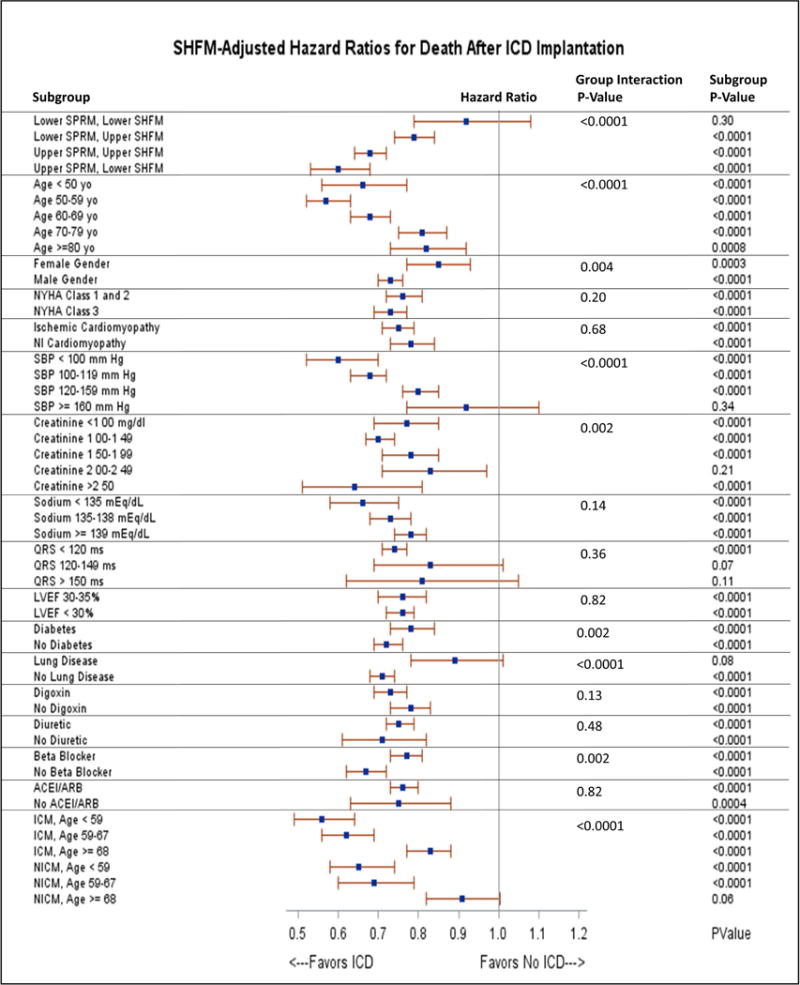
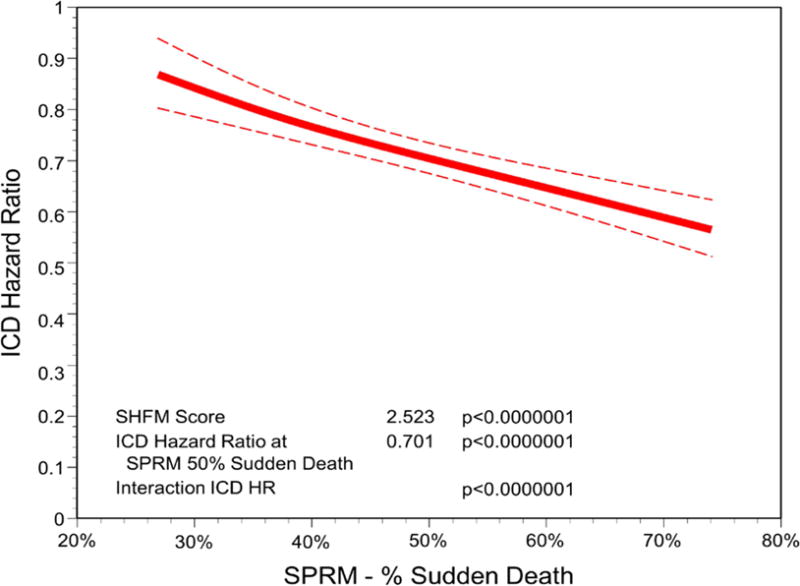
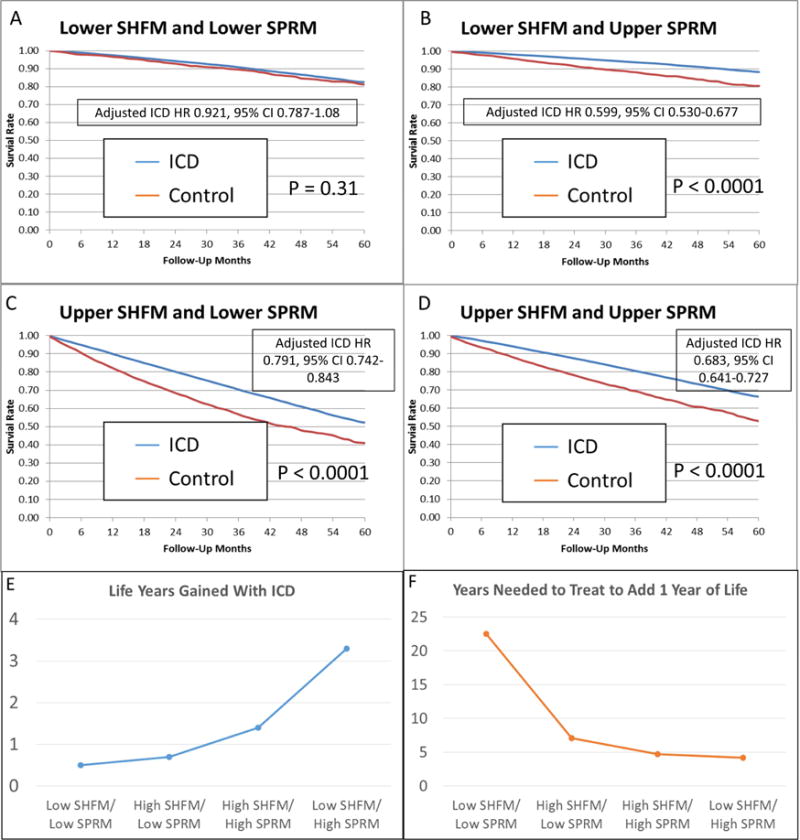
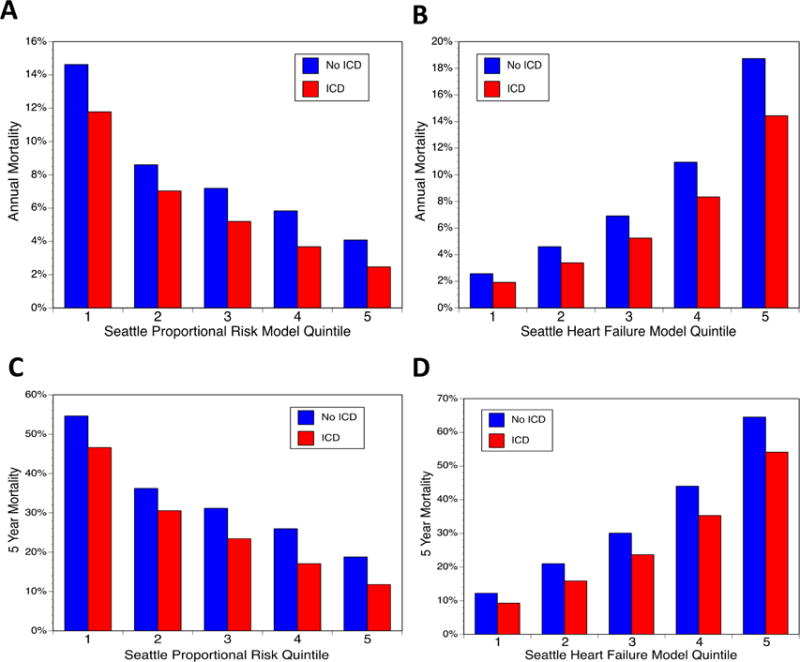
Results: Among 98,846 patients with HF (87,914 with ICDs and 10,932 without ICDs), the SHFM was strongly associated with all-cause mortality (p < 0.0001). The ICD-SPRM interaction was significant (p < 0.0001), such that SPRM quintile 5 patients had approximately twice the reduction in mortality with the ICD versus SPRM quintile 1 patients (adjusted hazard ratios [HR]: 0.602; 95% confidence interval [CI]: 0.537 to 0.675 vs. 0.793; 95% CI: 0.736 to 0.855, respectively). Among patients with SHFM-predicted annual mortality ≤5.7%, those with a SPRM-predicted risk of sudden death below the median had no reduction in mortality with the ICD (adjusted ICD HR: 0.921; 95% CI: 0.787 to 1.08; p = 0.31), whereas those with SPRM above the median derived the greatest benefit (adjusted HR: 0.599; 95% CI: 0.530 to 0.677; p < 0.0001).
Conclusions: The SHFM predicted all-cause mortality in a large cohort with and without ICDs, and the SPRM discriminated and calibrated the potential ICD benefit. Together, the models identified patients less likely to derive a survival benefit from primary prevention ICDs.
Keywords: heart failure; implantable cardioverter-defibrillator; risk models.
Copyright © 2017 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Who Benefits From Implantable Cardioverter-Defibrillators?: Integrating Absolute, Proportional, and Competing Risk.J Am Coll Cardiol. 2017 May 30;69(21):2619-2621. doi: 10.1016/j.jacc.2017.04.006. J Am Coll Cardiol. 2017. PMID: 28545634 No abstract available.
References
-
- Roger VL, Weston SA, Redfield MM, et al. Trends in heart failure incidence and survival in a community-based population. JAMA. 2004;292:344–50. - PubMed
-
- Levy D, Kenchaiah S, Larson MG, et al. Long-term trends in the incidence of and survival with heart failure. N Engl J Med. 2002;347:1397–402. - PubMed
-
- Haldeman GA, Croft JB, Giles WH, Rashidee A. Hospitalization of patients with heart failure: National Hospital Discharge Survey, 1985 to 1995. Am Heart J. 1999;137:352–60. - PubMed
-
- Bardy GH, Lee KL, Mark DB, et al. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N Engl J Med. 2005;352:225–37. - PubMed
-
- Moss AJ, Zareba W, Hall WJ, et al. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med. 2002;346:877–83. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
