

Tests for Serum Transglutaminase and Endomysial Antibodies Do Not Detect Most Patients With Celiac Disease and Persistent Villous Atrophy on Gluten-free Diets: a Meta-analysis
- PMID: 28545781
- PMCID: PMC5738024
- DOI: 10.1053/j.gastro.2017.05.015
Tests for Serum Transglutaminase and Endomysial Antibodies Do Not Detect Most Patients With Celiac Disease and Persistent Villous Atrophy on Gluten-free Diets: a Meta-analysis
Abstract
Background & aims: Tests to measure serum endomysial antibodies (EMA) and antibodies to tissue transglutaminase (tTG) were developed to screen for celiac disease in patients consuming gluten. However, they are commonly used to monitor patients on a gluten-free diet (GFD). We conducted a meta-analysis to assess the sensitivity and specificity of tTG IgA and EMA IgA assays in identifying patients with celiac disease who have persistent villous atrophy despite a GFD.
Methods: We searched PUBMED, EMBASE, BIOSIS, SCOPUS, clinicaltrials.gov, Science Citation Index, and Cochrane Library databases through November 2016. Inclusion criteria were studies of subjects with biopsy-confirmed celiac disease, follow-up biopsies, and measurement of serum antibodies on a GFD, biopsy performed on subjects regardless of symptoms, or antibody test results. Our analysis excluded subjects with refractory celiac disease, undergoing gluten challenge, or consuming a prescribed oats-containing GFD. Tests were considered to have positive or negative findings based on manufacturer cut-off values. Villous atrophy was defined as a Marsh 3 lesion or villous height:crypt depth ratio below 3.0. We constructed forest plots to determine the sensitivity and specificity of detection for individual studies. For the meta-analysis, a bivariate random effects model was used to jointly model sensitivity and specificity.
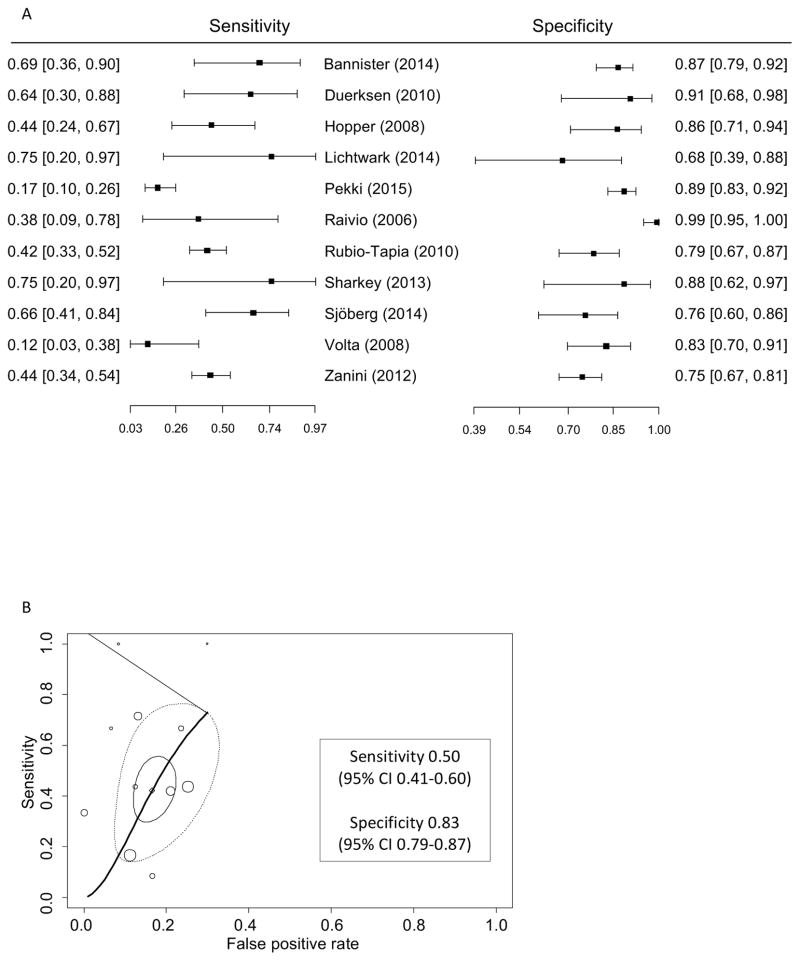
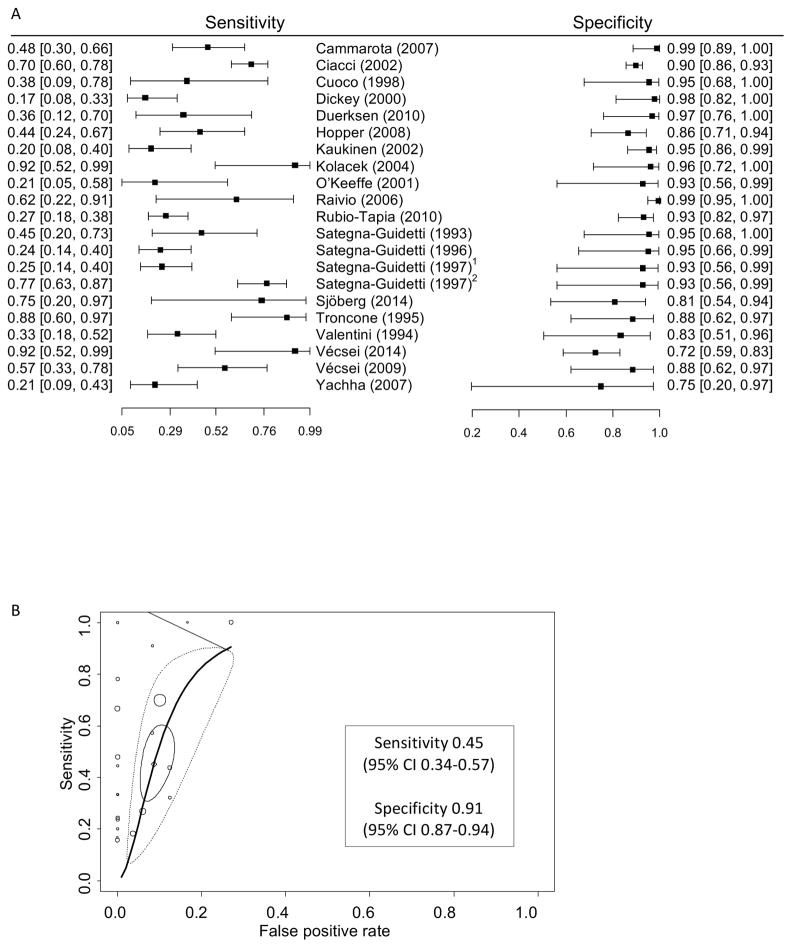
Results: Our search identified 5408 unique citations. Following review of abstracts, 442 articles were reviewed in detail. Only 26 studies (6 of tTG assays, 15 of EMA assays, and 5 of tTG and EMA assays) met our inclusion criteria. The most common reason studies were excluded from our analysis was inability to cross-tabulate histologic and serologic findings. The serum assays identified patients with persistent villous atrophy with high levels of specificity: 0.83 for the tTG IgA assay (95% CI, 0.79-0.87) and 0.91 for the EMA IgA assay (95% CI, 0.87-0.94). However, they detected villous atrophy with low levels of sensitivity: 0.50 for the tTG IgA assay (95% CI, 0.41-0.60) and 0.45 for the EMA IgA assay (95% CI, 0.34-0.57). The tests had similar levels of performance in pediatric and adult patients.
Conclusions: In a meta-analysis of patients with biopsy-confirmed celiac disease undergoing follow-up biopsy on a GFD, we found that tests for serum tTG IgA and EMA IgA levels had low sensitivity (below 50%) in detection of persistent villous atrophy. We need more-accurate non-invasive markers of mucosal damage in children and adults with celiac disease who are following a GFD.
Keywords: Endomysial Antibody; Monitoring and Follow-up Diagnostics; Tissue Transglutaminase Antibody.
Copyright © 2017 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Chorzelski TP, Beutner EH, Sulej J, et al. IgA anti-endomysium antibody. A new immunological marker of dermatitis herpetiformis and coeliac disease. Br J Dermatol. 1984;111:395–402. - PubMed
-
- Dieterich W, Ehnis T, Bauer M, et al. Identification of tissue transglutaminase as the autoantigen of celiac disease. Nat Med. 1997;3:797–801. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
