

Albuminuria, Proteinuria, and Renal Disease Progression in Children with CKD
- PMID: 28546440
- PMCID: PMC5460717
- DOI: 10.2215/CJN.11971116
Albuminuria, Proteinuria, and Renal Disease Progression in Children with CKD
Abstract
Background and objectives: The role of albuminuria as an indicator of progression has not been investigated in children with CKD in the absence of diabetes.
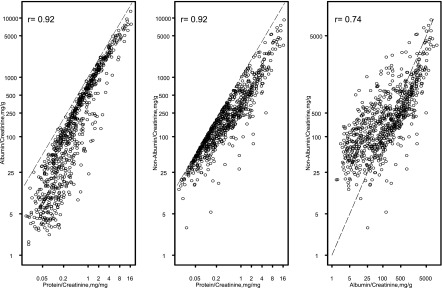
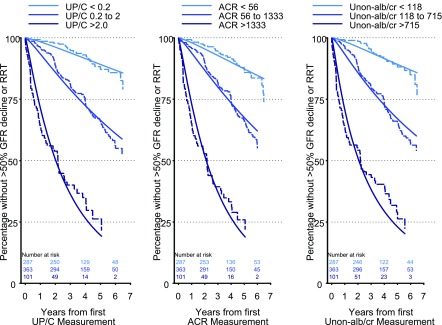
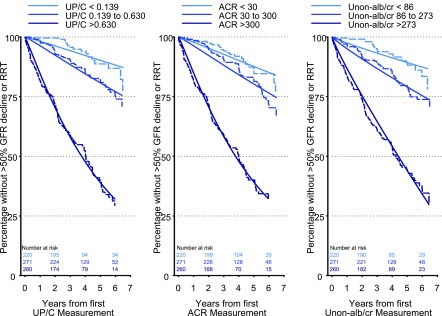
Design, setting, participants, & measurements: Children were enrolled from 49 centers of the CKD in Children study between January of 2005 and March of 2014. Cross-sectional multivariable linear regression (n=647) was used to examine the relationship between urine protein-to-creatinine (UP/C [milligrams per milligram]) and albumin-to-creatinine (ACR [milligrams per gram]) with eGFR (milliliters per minute per 1.73 m2). Parametric time-to-event analysis (n=751) was used to assess the association of UP/C, ACR, and urine nonalbumin-to-creatinine (Unon-alb/cr [milligrams per gram]) on the time to the composite endpoint of initiation of RRT or 50% decline in eGFR.
Results: The median follow-up time was 3.4 years and 202 individuals experienced the event. Participants with a UP/C≥0.2 mg/mg and ACR≥30 mg/g had a mean eGFR that was 16 ml/min per 1.73 m2 lower than those with a UP/C<0.2 mg/mg and ACR<30 mg/g. Individuals with ACR<30 mg/g, but a UP/C≥0.2 mg/mg, had a mean eGFR that was 9.3 ml/min per 1.73 m2 lower than those with a UP/C<0.2 mg/mg and ACR<30 mg/g. When categories of ACR and Unon-alb/cr were created on the basis of clinically meaningful cutoff values of UP/C with the same sample sizes for comparison, the relative times (RTs) to the composite end-point were almost identical when comparing the middle (RT=0.31 for UP/C [0.2-2.0 mg/mg], RT=0.38 for ACR [56-1333 mg/g], RT=0.31 for Unon-alb/cr [118-715 mg/g]) and the highest (RT=0.08 for UP/C [>2.0 mg/mg], RT=0.09 for ACR [>1333 mg/g], RT=0.07 for Unon-alb/cr [>715 mg/g]) levels to the lowest levels. A similar trend was seen when categories were created on the basis of clinically meaningful cutoff values of ACR (<30, 30-300, >300 mg/g).
Conclusions: In children with CKD without diabetes, the utility of an initial UP/C, ACR, and Unon-alb/cr for characterizing progression is similar.
Keywords: Cross-Sectional Studies; Disease Progression; Follow-Up Studies; Humans; Linear Models; Renal Insufficiency, Chronic; Renal Replacement Therapy; Sample Size; albuminuria; creatinine; diabetes mellitus; glomerular filtration rate; kidney; pediatrics; progression of chronic renal failure; proteinuria; renal function decline.
Copyright © 2017 by the American Society of Nephrology.
Figures
References
-
- Warady BA, Abraham AG, Schwartz GJ, Wong CS, Muñoz A, Betoko A, Mitsnefes M, Kaskel F, Greenbaum LA, Mak RH, Flynn J, Moxey-Mims MM, Furth S: Predictors of rapid progression of glomerular and nonglomerular kidney disease in children and adolescents: The chronic kidney disease in children (CKiD) cohort. Am J Kidney Dis 65: 878–888, 2015 - PMC - PubMed
-
- Wühl E, Trivelli A, Picca S, Litwin M, Peco-Antic A, Zurowska A, Testa S, Jankauskiene A, Emre S, Caldas-Afonso A, Anarat A, Niaudet P, Mir S, Bakkaloglu A, Enke B, Montini G, Wingen AM, Sallay P, Jeck N, Berg U, Caliskan S, Wygoda S, Hohbach-Hohenfellner K, Dusek J, Urasinski T, Arbeiter K, Neuhaus T, Gellermann J, Drozdz D, Fischbach M, Möller K, Wigger M, Peruzzi L, Mehls O, Schaefer F; ESCAPE Trial Group : Strict blood-pressure control and progression of renal failure in children. N Engl J Med 361: 1639–1650, 2009 - PubMed
-
- Levin A, Stevens PE: Summary of KDIGO 2012 CKD Guideline: Behind the scenes, need for guidance, and a framework for moving forward. Kidney Int 85: 49–61, 2014 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
