

Classification of Paediatric Inflammatory Bowel Disease using Machine Learning
- PMID: 28546534
- PMCID: PMC5445076
- DOI: 10.1038/s41598-017-02606-2
Classification of Paediatric Inflammatory Bowel Disease using Machine Learning
Abstract
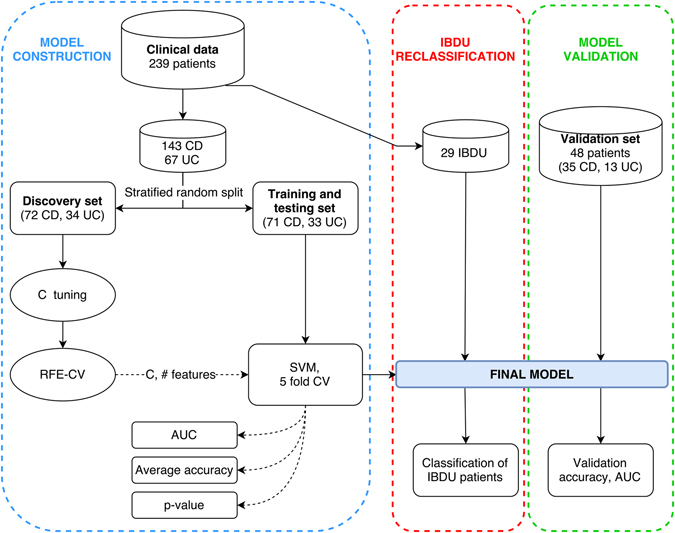
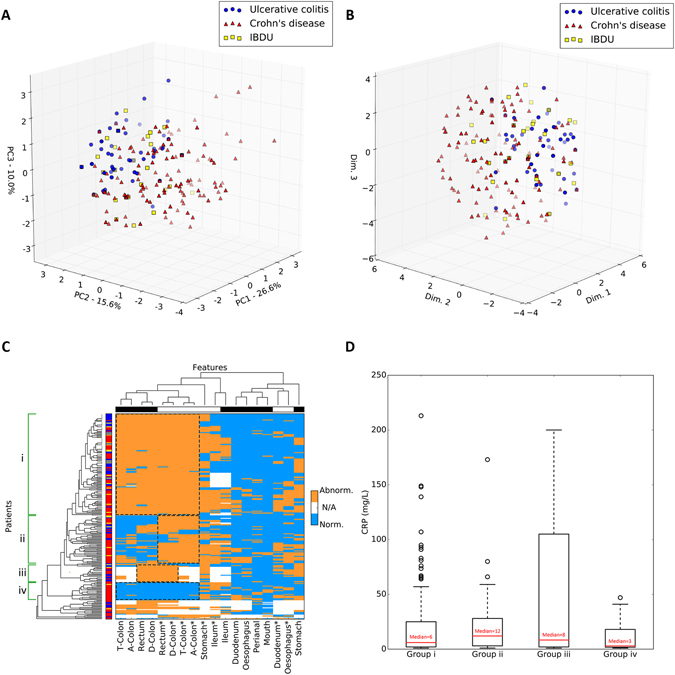
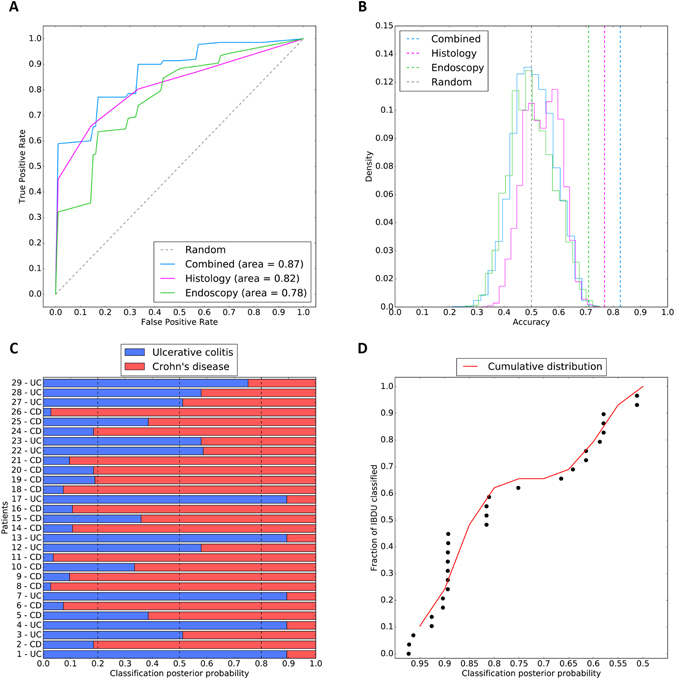
Paediatric inflammatory bowel disease (PIBD), comprising Crohn's disease (CD), ulcerative colitis (UC) and inflammatory bowel disease unclassified (IBDU) is a complex and multifactorial condition with increasing incidence. An accurate diagnosis of PIBD is necessary for a prompt and effective treatment. This study utilises machine learning (ML) to classify disease using endoscopic and histological data for 287 children diagnosed with PIBD. Data were used to develop, train, test and validate a ML model to classify disease subtype. Unsupervised models revealed overlap of CD/UC with broad clustering but no clear subtype delineation, whereas hierarchical clustering identified four novel subgroups characterised by differing colonic involvement. Three supervised ML models were developed utilising endoscopic data only, histological only and combined endoscopic/histological data yielding classification accuracy of 71.0%, 76.9% and 82.7% respectively. The optimal combined model was tested on a statistically independent cohort of 48 PIBD patients from the same clinic, accurately classifying 83.3% of patients. This study employs mathematical modelling of endoscopic and histological data to aid diagnostic accuracy. While unsupervised modelling categorises patients into four subgroups, supervised approaches confirm the need of both endoscopic and histological evidence for an accurate diagnosis. Overall, this paper provides a blueprint for ML use with clinical data.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Accurate Classification of Pediatric Colonic Inflammatory Bowel Disease Subtype Using a Random Forest Machine Learning Classifier.J Pediatr Gastroenterol Nutr. 2021 Feb 1;72(2):262-269. doi: 10.1097/MPG.0000000000002956. J Pediatr Gastroenterol Nutr. 2021. PMID: 33003163
-
Appraisal of the PIBD-classes Criteria: A Multicentre Validation.J Crohns Colitis. 2020 Dec 2;14(12):1672-1679. doi: 10.1093/ecco-jcc/jjaa103. J Crohns Colitis. 2020. PMID: 32453831
-
[Application of the Porto criteria for the diagnosis of paediatric inflammatory bowel disease in a paediatric reference centre].An Pediatr (Barc). 2011 Oct;75(4):232-8. doi: 10.1016/j.anpedi.2011.03.011. Epub 2011 May 5. An Pediatr (Barc). 2011. PMID: 21549650 Spanish.
-
Paediatric inflammatory bowel disease: review with a focus on practice in low- to middle-income countries.Paediatr Int Child Health. 2019 Feb;39(1):48-58. doi: 10.1080/20469047.2019.1575056. Paediatr Int Child Health. 2019. PMID: 30900526 Review.
-
SYSTEMATIC REVIEW AND META - ANALYSIS OF THE FREQUENCY AND RE-CLASSIFICATION TRENDS OF PEDIATRIC INFLAMMATORY BOWEL DISEASE - UNCLASSIFIED.Arq Gastroenterol. 2022 Oct-Dec;59(4):531-539. doi: 10.1590/S0004-2803.202204000-92. Arq Gastroenterol. 2022. PMID: 36515348
Cited by
-
Diagnosis of Crohn's disease and ulcerative colitis using the microbiome.BMC Microbiol. 2023 Nov 11;23(1):336. doi: 10.1186/s12866-023-03084-5. BMC Microbiol. 2023. PMID: 37951857 Free PMC article.
-
Identifying heterogeneous subgroups of systemic autoimmune diseases by applying a joint dimension reduction and clustering approach to immunomarkers.BioData Min. 2024 Sep 16;17(1):36. doi: 10.1186/s13040-024-00389-7. BioData Min. 2024. PMID: 39285420 Free PMC article.
-
Gut microbiota analysis for prediction of clinical relapse in Crohn's disease.Sci Rep. 2022 Nov 19;12(1):19929. doi: 10.1038/s41598-022-23757-x. Sci Rep. 2022. PMID: 36402792 Free PMC article.
-
A Systematic Review of Artificial Intelligence and Machine Learning Applications to Inflammatory Bowel Disease, with Practical Guidelines for Interpretation.Inflamm Bowel Dis. 2022 Oct 3;28(10):1573-1583. doi: 10.1093/ibd/izac115. Inflamm Bowel Dis. 2022. PMID: 35699597 Free PMC article.
-
A Review of Colonoscopy in Intestinal Diseases.Diagnostics (Basel). 2023 Mar 27;13(7):1262. doi: 10.3390/diagnostics13071262. Diagnostics (Basel). 2023. PMID: 37046479 Free PMC article. Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
