

Salvage Surgery for Cervical Cancer Recurrences
- PMID: 28546709
- PMCID: PMC5427013
- DOI: 10.1007/s13193-015-0472-2
Salvage Surgery for Cervical Cancer Recurrences
Abstract
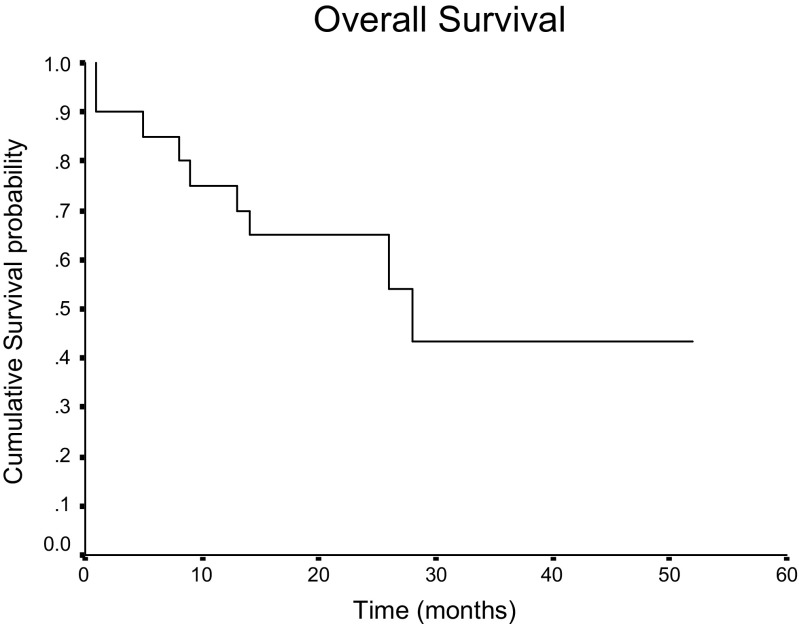
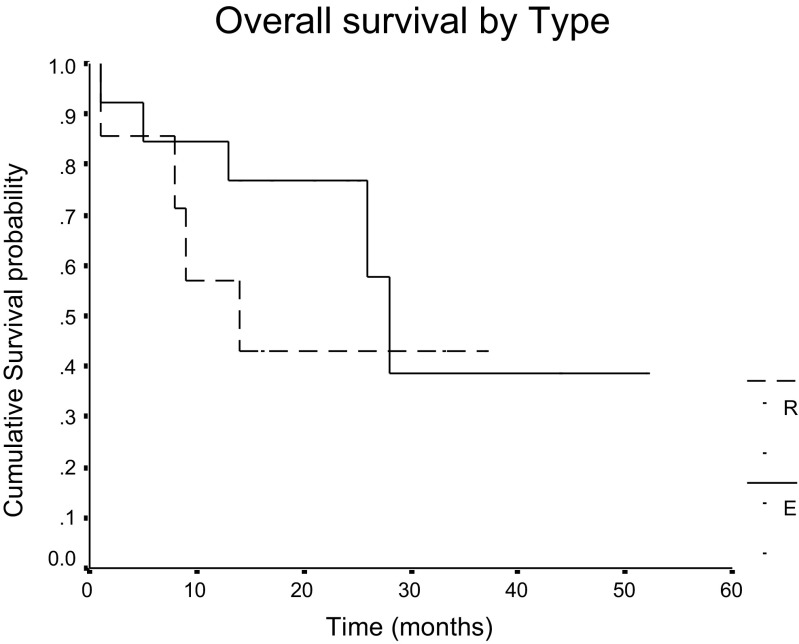
Cervical cancer usually presents in advanced stages and is treated with chemoradiation. About 15-20 % patients present with local recurrence after chemoradiation. Radical surgical resection is the only treatment modality offering long term survival benefit in recurrent cervical cancer. The most common surgical option for these patients is pelvic exenteration. Radical hysterectomy may be done for patients with a small centrally located recurrence in the cervix with no infiltration of adjacent structures. The aim of this study was to evaluate the morbidity and survival outcome following radical hysterectomy and pelvic exenteration for recurrent cancer cervix. We retrospectively reviewed the medical records of our patients who underwent surgery for cancer cervix recurrence from January 2010 to December 2014. The postoperative morbidity was considered early if it happened in the initial 30 days of surgery and late if it occurred after 30 days. All patients were followed up till February 2015. Survival analysis was done using Kaplan- Meir method. Between January 2010 and December 2014, 20 patients with recurrent cervical cancer underwent radical surgical resection. The median age of the study group was 43 years (range 28-63 years). Seventeen patients had squamous cell carcinoma and 3 had adenocarcinoma. 13 underwent pelvic exenteration and 7 patients underwent radical type 2 hysterectomy with bilateral pelvic lymphnode dissection. In the exenteration group, 8 patients had anterior exenteration, 4 had total exenteration and one had posterior exenteration. Urinary diversion was done by ileal conduit in 8 patients, double barrel colostomy in two and wet colostomy in two patients. There were no immediate postoperative deaths. Operating time, blood transfusions needed and hospital stay was more in the exenteration group compared to radical hysterectomy patients. After pelvic exenteration post-operative complications were seen in 76.9 % of which the most common was of the urinary tract including 3 patients with pyelonephritis, 5 had renal insufficiency and 2 patients developed urinary fistulae. Post-operative morbidity was lower in radical hysterectomy patients. There were two patients in the hysterectomy group who developed vault recurrence while none in the exenteration group had local recurrence. The median follow up time was 19 months (range 9-53 months).Three year overall survival for the entire cohort was 43 %. Median survival time for the exenteration group was 28 months which was significantly higher than 14 months for the radical hysterectomy group. This study shows that radical surgical resection is feasible with good survival outcome and acceptable morbidity in recurrent cancer cervix patients. Radical hysterectomy can be done in selected patients but pelvic exenteration has better long-term survival but with the potential for both short- & long-term complications.
Keywords: Cancer cervix recurrence; Morbidity; Pelvic exenteration; Salvage hysterectomy; Salvage surgery.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources