

The Epidemiology of Hospital Death Following Pediatric Severe Sepsis: When, Why, and How Children With Sepsis Die
- PMID: 28549024
- PMCID: PMC5581233
- DOI: 10.1097/PCC.0000000000001222
The Epidemiology of Hospital Death Following Pediatric Severe Sepsis: When, Why, and How Children With Sepsis Die
Abstract
Objective: The epidemiology of in-hospital death after pediatric sepsis has not been well characterized. We investigated the timing, cause, mode, and attribution of death in children with severe sepsis, hypothesizing that refractory shock leading to early death is rare in the current era.
Design: Retrospective observational study.
Setting: Emergency departments and ICUs at two academic children's hospitals.
Patients: Seventy-nine patients less than 18 years old treated for severe sepsis/septic shock in 2012-2013 who died prior to hospital discharge.
Interventions: None.
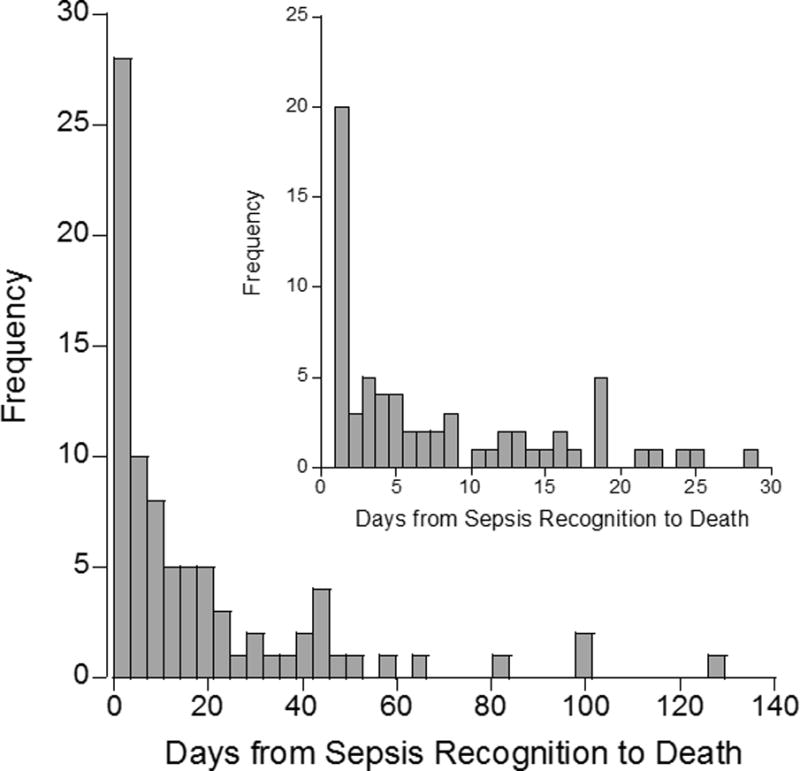
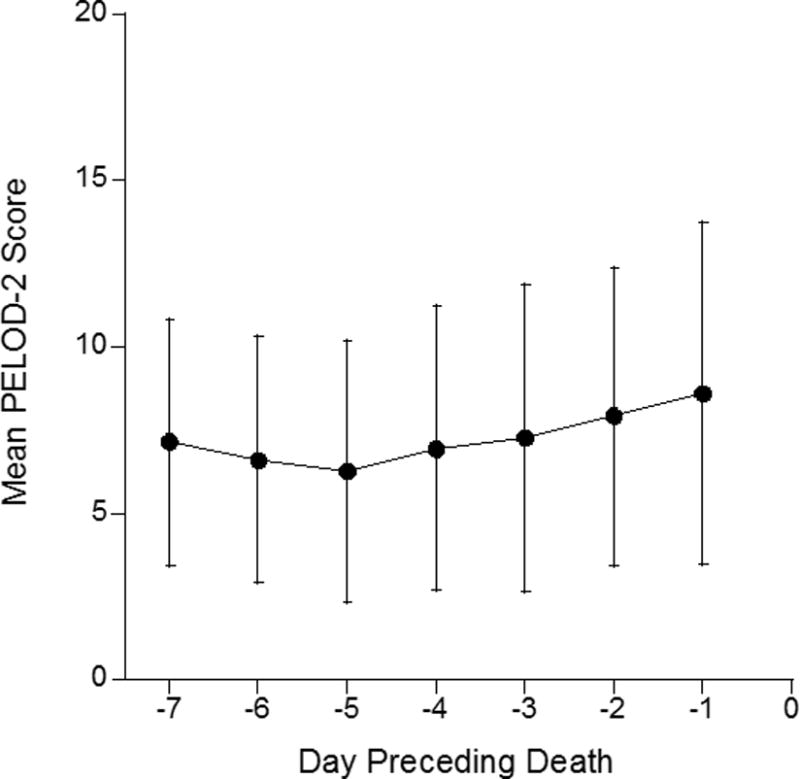
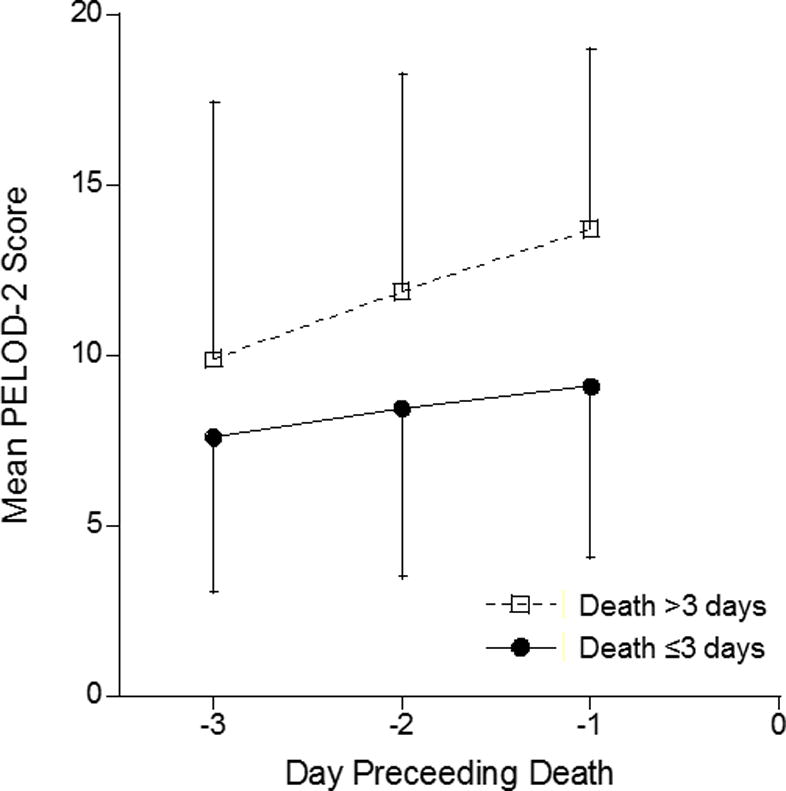
Measurements and main results: Time to death from sepsis recognition, cause and mode of death, and attribution of death to sepsis were determined from medical records. Organ dysfunction was assessed via daily Pediatric Logistic Organ Dysfunction-2 scores for 7 days preceding death with an increase greater than or equal to 5 defined as worsening organ dysfunction. The median time to death was 8 days (interquartile range, 1-12 d) with 25%, 35%, and 49% of cumulative deaths within 1, 3, and 7 days of sepsis recognition, respectively. The most common cause of death was refractory shock (34%), then multiple organ dysfunction syndrome after shock recovery (27%), neurologic injury (19%), single-organ respiratory failure (9%), and nonseptic comorbidity (6%). Early deaths (≤ 3 d) were mostly due to refractory shock in young, previously healthy patients while multiple organ dysfunction syndrome predominated after 3 days. Mode of death was withdrawal in 72%, unsuccessful cardiopulmonary resuscitation in 22%, and irreversible loss of neurologic function in 6%. Ninety percent of deaths were attributable to acute or chronic manifestations of sepsis. Only 23% had a rise in Pediatric Logistic Organ Dysfunction-2 that indicated worsening organ dysfunction.
Conclusions: Refractory shock remains a common cause of death in pediatric sepsis, especially for early deaths. Later deaths were mostly attributable to multiple organ dysfunction syndrome, neurologic, and respiratory failure after life-sustaining therapies were limited. A pattern of persistent, rather than worsening, organ dysfunction preceded most deaths.
Conflict of interest statement
The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Comment in
-
Early Death From Pediatric Severe Sepsis: Still a Problem and a Mandate for Future Clinical Research.Pediatr Crit Care Med. 2017 Sep;18(9):891-892. doi: 10.1097/PCC.0000000000001239. Pediatr Crit Care Med. 2017. PMID: 28863088 No abstract available.
References
-
- Hartman ME, Linde-Zwirble WT, Angus DC, et al. Trends in the Epidemiology of Pediatric Severe Sepsis. Pediatr Crit Care Med. 2013;14(7):868–693. - PubMed
-
- Wang H, Dwyer-Lindgren L, Lofgren KT, et al. Age-specific and sex-specific mortality in 187 countries, 1970–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2071–2094. - PubMed
-
- Vincent JL, Nelson DR, Williams MD. Is worsening multiple organ failure the cause of death in patients with severe sepsis? Crit Care Med. 2011;39(5):1050–1055. - PubMed
-
- Curley MA, Zimmerman JJ. Alternative outcome measures for pediatric clinical sepsis trials. Pediatr Crit Care Med. 2005;6(3 Suppl):S150–156. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
