

Characteristics associated with quality of life among people with drug-resistant epilepsy
- PMID: 28550480
- PMCID: PMC5486549
- DOI: 10.1007/s00415-017-8512-1
Characteristics associated with quality of life among people with drug-resistant epilepsy
Abstract
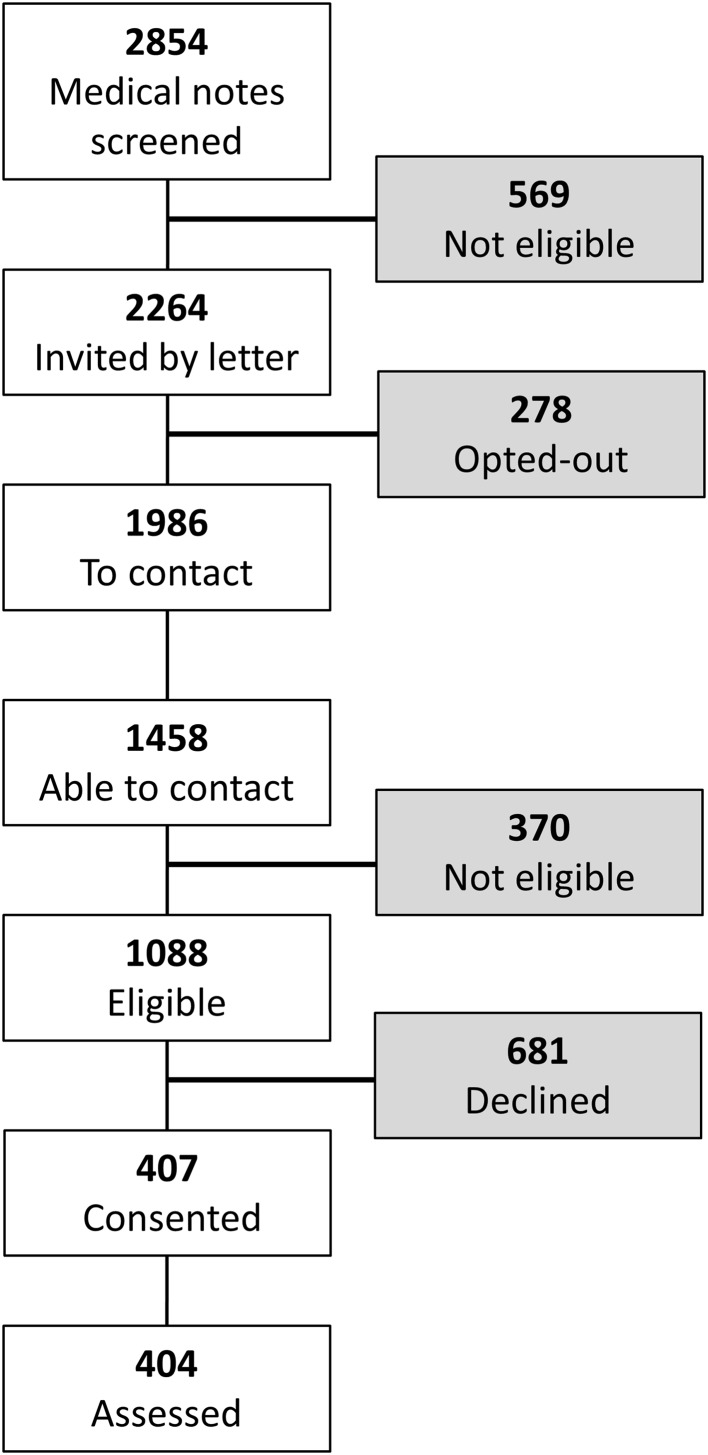
Quality of Life (QoL) is the preferred outcome in non-pharmacological trials, but there is little UK population evidence of QoL in epilepsy. In advance of evaluating an epilepsy self-management course we aimed to describe, among UK participants, what clinical and psycho-social characteristics are associated with QoL. We recruited 404 adults attending specialist clinics, with at least two seizures in the prior year and measured their self-reported seizure frequency, co-morbidity, psychological distress, social characteristics, including self-mastery and stigma, and epilepsy-specific QoL (QOLIE-31-P). Mean age was 42 years, 54% were female, and 75% white. Median time since diagnosis was 18 years, and 69% experienced ≥10 seizures in the prior year. Nearly half (46%) reported additional medical or psychiatric conditions, 54% reported current anxiety and 28% reported current depression symptoms at borderline or case level, with 63% reporting felt stigma. While a maximum QOLIE-31-P score is 100, participants' mean score was 66, with a wide range (25-99). In order of large to small magnitude: depression, low self-mastery, anxiety, felt stigma, a history of medical and psychiatric comorbidity, low self-reported medication adherence, and greater seizure frequency were associated with low QOLIE-31-P scores. Despite specialist care, UK people with epilepsy and persistent seizures experience low QoL. If QoL is the main outcome in epilepsy trials, developing and evaluating ways to reduce psychological and social disadvantage are likely to be of primary importance. Educational courses may not change QoL, but be one component supporting self-management for people with long-term conditions, like epilepsy.
Keywords: Anxiety; Depression; Epilepsy; Quality of life; Self-mastery; Stigma.
Conflict of interest statement
Conflicts of interest
The authors have no conflicts of interest.
Ethical standards
This study was approved by the National Research Ethics Service Committee London—Fulham (REC reference 12/LO/1962) and was performed by the ethical standards laid down in the 1964 Declaration of Helsinki, and its later amendments. All participants, themselves, gave their written consent prior to enrolment.
Figures

References
-
- Moran N, Poole K, Bell G, Solomon J, Kendall S, McCarthy M, McCormick D, Nashef L, Johnson A, Sander J, Shorvon S. NHS services for epilepsy from the patient’s perspective: a survey of primary, secondary and tertiary care access throughout the UK. Seizure. 2000;9(8):559–565. doi: 10.1053/seiz.2000.0451. - DOI - PubMed
-
- Ridsdale L. Avoiding premature death in epilepsy. BMJ. 2015 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
