

Previous radiotherapy and the clinical activity and toxicity of pembrolizumab in the treatment of non-small-cell lung cancer: a secondary analysis of the KEYNOTE-001 phase 1 trial
- PMID: 28551359
- PMCID: PMC5538772
- DOI: 10.1016/S1470-2045(17)30380-7
Previous radiotherapy and the clinical activity and toxicity of pembrolizumab in the treatment of non-small-cell lung cancer: a secondary analysis of the KEYNOTE-001 phase 1 trial
Erratum in
-
Correction to Lancet Oncol 2017; 18: 895-903.Lancet Oncol. 2017 Jul;18(7):e371. doi: 10.1016/S1470-2045(17)30409-6. Epub 2017 May 25. Lancet Oncol. 2017. PMID: 28552211 No abstract available.
Abstract
Background: Preclinical studies have found radiotherapy enhances antitumour immune responses. We aimed to assess disease control and pulmonary toxicity in patients who previously received radiotherapy for non-small-cell lung cancer (NSCLC) before receiving pembrolizumab.
Methods: We assessed patients with advanced NSCLC treated on the phase 1 KEYNOTE-001 trial at a single institution (University of California, Los Angeles, CA, USA). Patients were aged 18 years or older, had an Eastern Cooperative Oncology Group performance status of 1 or less, had adequate organ function, and no history of pneumonitis. Patients received pembrolizumab at a dose of either 2 mg/kg of bodyweight or 10 mg/kg every 3 weeks, or 10 mg/kg every 2 weeks, until disease progression, unacceptable toxicity, or other protocol-defined reasons for discontinuation. Disease response and pulmonary toxicity were prospectively assessed by Immune-related Response Criteria and Common Terminology Criteria for Adverse Events version 4.0. The primary objective of the KEYNOTE-001 trial was to assess the safety, side-effect profile, and antitumour activity of pembrolizumab. For our secondary analysis, patients were divided into subgroups to compare patients who previously received radiotherapy with patients who had not. Our primary objective was to determine whether previous radiotherapy affected progression-free survival, overall survival, and pulmonary toxicity in the intention-to-treat population. The KEYNOTE-001 trial was registered with ClinicalTrials.gov, number NCT01295827.
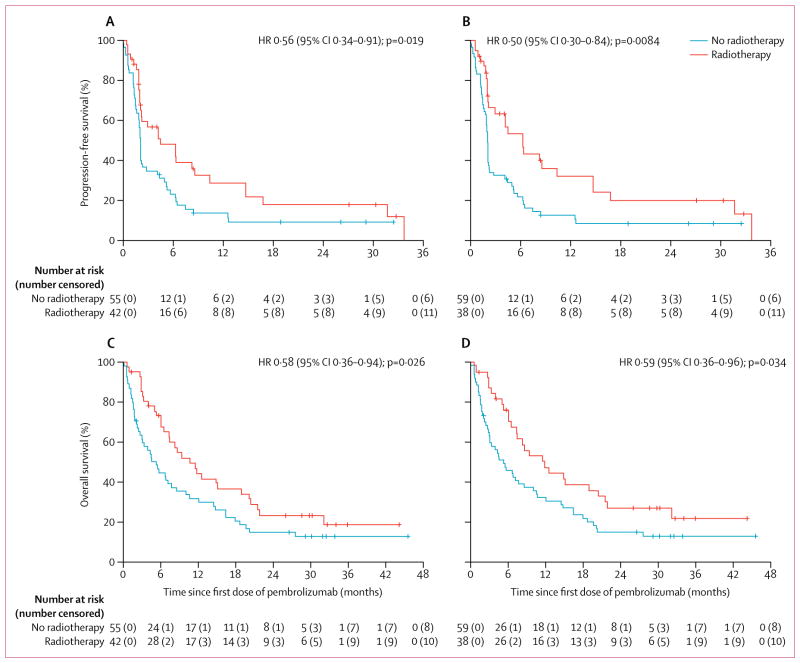
Findings: Between May 22, 2012, and July 11, 2014, 98 patients were enrolled and received their first cycle of pembrolizumab. One patient was lost to follow-up. 42 (43%) of 97 patients had previously received any radiotherapy for the treatment of NSCLC before the first cycle of pembrolizumab. 38 (39%) of 97 patients received extracranial radiotherapy and 24 (25%) of 97 patients received thoracic radiotherapy. Median follow-up for surviving patients was 32·5 months (IQR 29·8-34·1). Progression-free survival with pembrolizumab was significantly longer in patients who previously received any radiotherapy than in patients without previous radiotherapy (hazard ratio [HR] 0·56 [95% CI 0·34-0·91], p=0·019; median progression-free survival 4·4 months [95% CI 2·1-8·6] vs 2·1 months [1·6-2·3]) and for patients who previously received extracranial radiotherapy compared with those without previous extracranial radiotherapy (HR 0·50 [0·30-0·84], p=0·0084; median progression-free survival 6·3 months [95% CI 2·1-10·4] vs 2·0 months [1·8-2·1]). Overall survival with pembrolizumab was significantly longer in patients who previously received any radiotherapy than in patients without previous radiotherapy (HR 0·58 [95% CI 0·36-0·94], p=0·026; median overall survival 10·7 months [95% CI 6·5-18·9] vs 5·3 months [2·7-7·7]) and for patients who previously received extracranial radiotherapy compared with those without previous extracranial radiotherapy (0·59 [95% CI 0·36-0·96], p=0·034; median overall survival 11·6 months [95% CI 6·5-20·5] vs 5·3 months [3·0-8·5]). 15 (63%) of 24 patients who had previously received thoracic radiotherapy had any recorded pulmonary toxicity versus 29 (40%) of 73 patients with no previous thoracic radiotherapy. Three (13%) patients with previous thoracic radiotherapy had treatment-related pulmonary toxicity compared with one (1%) of those without; frequency of grade 3 or worse treatment-related pulmonary toxicities was similar (one patient in each group).
Interpretation: Our data suggest that previous treatment with radiotherapy in patients with advanced NSCLC results in longer progression-free survival and overall survival with pembrolizumab treatment than that seen in patients who did not have previous radiotherapy, with an acceptable safety profile. Further clinical trials investigating this combination are needed to determine the optimal treatment strategy for patients with advanced NSCLC.
Funding: US National Institutes of Health.
Copyright © 2017 Elsevier Ltd. All rights reserved.
Conflict of interest statement
EBG reports grants from Merck during the conduct of the KEYNOTE-001 study; grants from AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Eli Lilly, Genentech, Mirati, Pfizer, and Novartis outside the submitted work. All other authors declare no competing interests.
Figures
Comment in
-
Radiotherapy and PD-L1 inhibition in metastatic NSCLC.Lancet Oncol. 2017 Jul;18(7):840-842. doi: 10.1016/S1470-2045(17)30354-6. Epub 2017 May 24. Lancet Oncol. 2017. PMID: 28551358 No abstract available.
-
Lung cancer: KEYNOTE-001 - combo improves melody.Nat Rev Clin Oncol. 2017 Jul;14(7):392-393. doi: 10.1038/nrclinonc.2017.85. Epub 2017 Jun 13. Nat Rev Clin Oncol. 2017. PMID: 28607520 No abstract available.
-
[Radiotherapy enhances the effect of PD-1 checkpoint inhibitors].Strahlenther Onkol. 2017 Sep;193(9):763-764. doi: 10.1007/s00066-017-1179-9. Strahlenther Onkol. 2017. PMID: 28698902 German. No abstract available.
-
Why is survival after pembrolizumab affected by previous radiotherapy?Lancet Oncol. 2017 Sep;18(9):e504. doi: 10.1016/S1470-2045(17)30472-2. Lancet Oncol. 2017. PMID: 28884692 No abstract available.
-
Why is survival after pembrolizumab affected by previous radiotherapy? - Authors' reply.Lancet Oncol. 2017 Sep;18(9):e505. doi: 10.1016/S1470-2045(17)30588-0. Lancet Oncol. 2017. PMID: 28884693 No abstract available.
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016;66:7–30. - PubMed
-
- Garon EB, Rizvi NA, Hui R, et al. Pembrolizumab for the of non-small-cell lung cancer. N Engl J Med. 2015;372:2018–28. - PubMed
-
- Reck M, Rodriguez-Abreu D, Robinson AG, et al. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N Engl J Med. 2016;375:1823–33. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
