

Heat and moisture exchangers (HMEs) and heated humidifiers (HHs) in adult critically ill patients: a systematic review, meta-analysis and meta-regression of randomized controlled trials
- PMID: 28552074
- PMCID: PMC5447307
- DOI: 10.1186/s13054-017-1710-5
Heat and moisture exchangers (HMEs) and heated humidifiers (HHs) in adult critically ill patients: a systematic review, meta-analysis and meta-regression of randomized controlled trials
Abstract
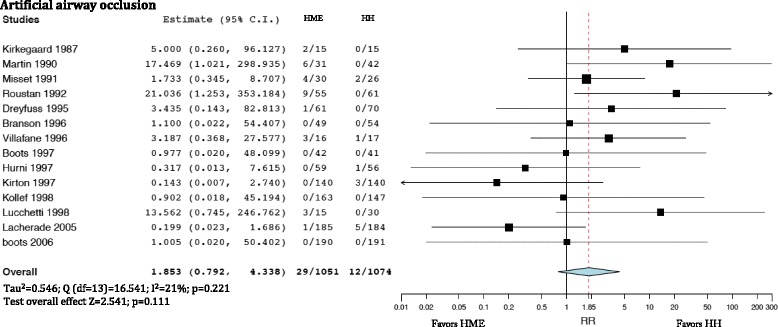
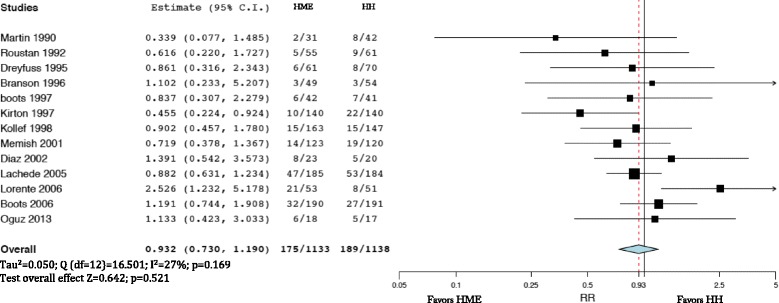
Background: The aims of this systematic review and meta-analysis of randomized controlled trials are to evaluate the effects of active heated humidifiers (HHs) and moisture exchangers (HMEs) in preventing artificial airway occlusion and pneumonia, and on mortality in adult critically ill patients. In addition, we planned to perform a meta-regression analysis to evaluate the relationship between the incidence of artificial airway occlusion, pneumonia and mortality and clinical features of adult critically ill patients.
Methods: Computerized databases were searched for randomized controlled trials (RCTs) comparing HHs and HMEs and reporting artificial airway occlusion, pneumonia and mortality as predefined outcomes. Relative risk (RR), 95% confidence interval for each outcome and I 2 were estimated for each outcome. Furthermore, weighted random-effect meta-regression analysis was performed to test the relationship between the effect size on each considered outcome and covariates.
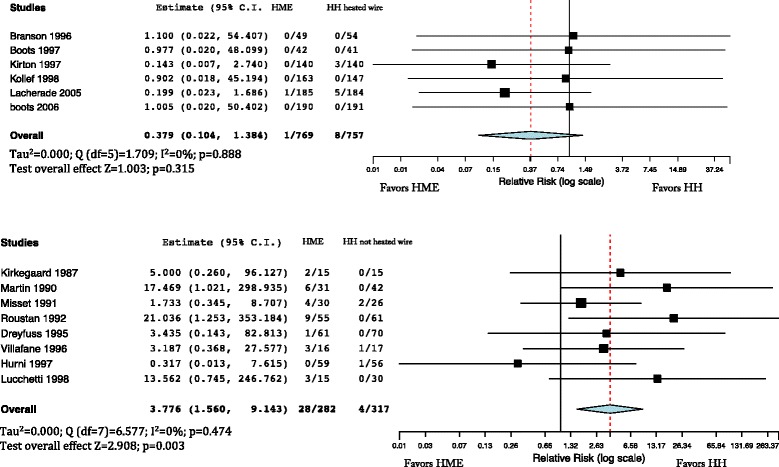
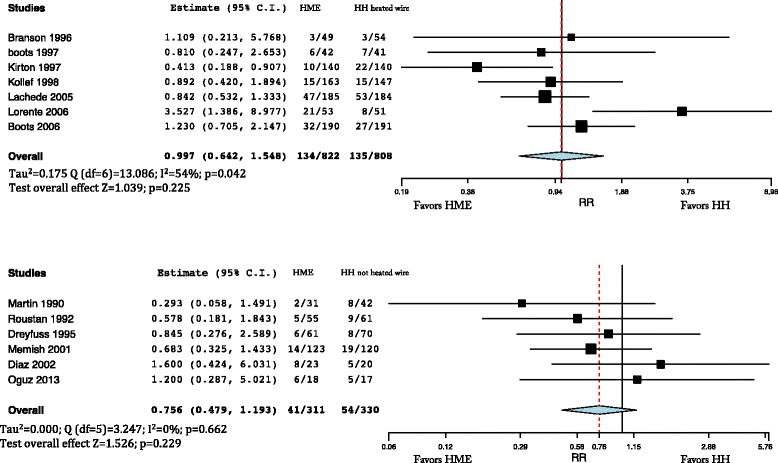
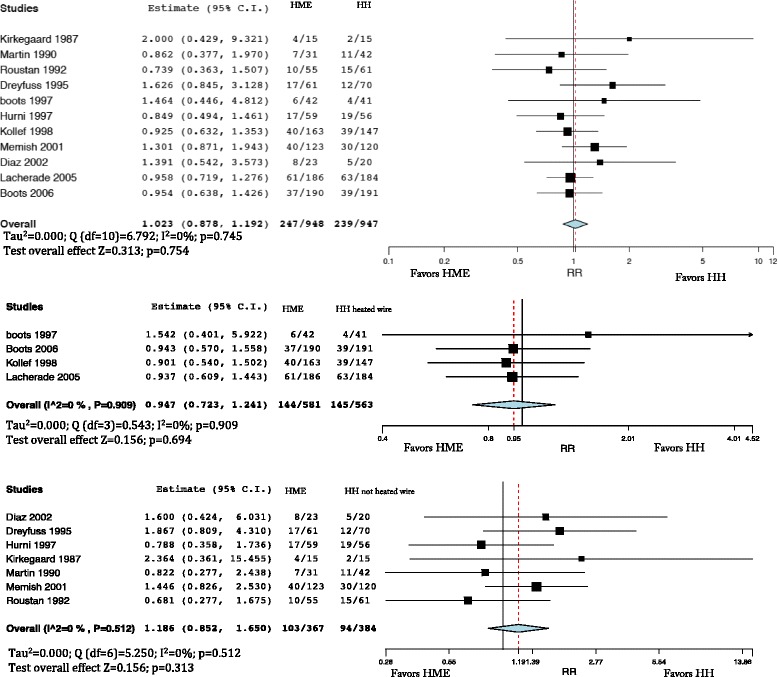
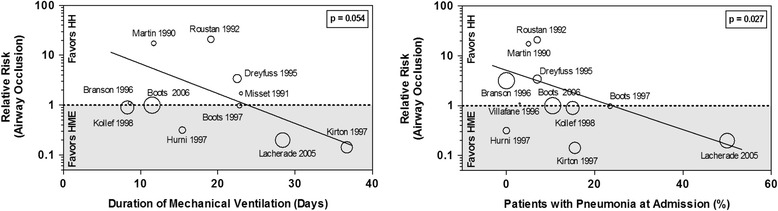
Results: Eighteen RCTs and 2442 adult critically ill patients were included in the analysis. The incidence of artificial airway occlusion (RR = 1.853; 95% CI 0.792-4.338), pneumonia (RR = 932; 95% CI 0.730-1.190) and mortality (RR = 1.023; 95% CI 0.878-1.192) were not different in patients treated with HMEs and HHs. However, in the subgroup analyses the incidence of airway occlusion was higher in HMEs compared with HHs with non-heated wire (RR = 3.776; 95% CI 1.560-9.143). According to the meta-regression, the effect size in the treatment group on artificial airway occlusion was influenced by the percentage of patients with pneumonia (β = -0.058; p = 0.027; favors HMEs in studies with high prevalence of pneumonia), and a trend was observed for an effect of the duration of mechanical ventilation (MV) (β = -0.108; p = 0.054; favors HMEs in studies with longer MV time).
Conclusions: In this meta-analysis we found no superiority of HMEs and HHs, in terms of artificial airway occlusion, pneumonia and mortality. A trend favoring HMEs was observed in studies including a high percentage of patients with pneumonia diagnosis at admission and those with prolonged MV. However, the choice of humidifiers should be made according to the clinical context, trying to avoid possible complications and reaching the appropriate performance at lower costs.
Keywords: Artificial airway occlusion; Heat and moisture exchangers; Heated humidifiers; Mortality; Pneumonia.
Figures
References
-
- Branson RD, Chatburn RL. Humidification of inspired gases during mechanical ventilation. Respir Care. 1993;38:461–8.
-
- Kelly M, Gillies D, Todd DA, Lockwood C. Heated humidification versus heat and moisture exchangers for ventilated adults and children. Cochrane Database Syst Rev. 2010;4:CD004711. doi:10.1002/14651858.CD004711.pub2. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
