

Optimising cluster survey design for planning schistosomiasis preventive chemotherapy
- PMID: 28552961
- PMCID: PMC5464666
- DOI: 10.1371/journal.pntd.0005599
Optimising cluster survey design for planning schistosomiasis preventive chemotherapy
Abstract
Background: The cornerstone of current schistosomiasis control programmes is delivery of praziquantel to at-risk populations. Such preventive chemotherapy requires accurate information on the geographic distribution of infection, yet the performance of alternative survey designs for estimating prevalence and converting this into treatment decisions has not been thoroughly evaluated.
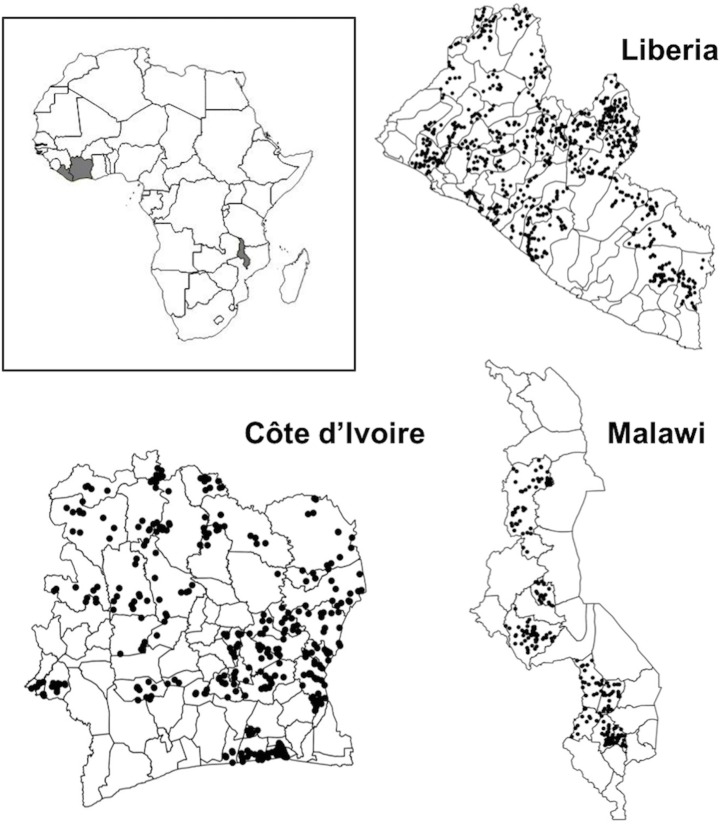
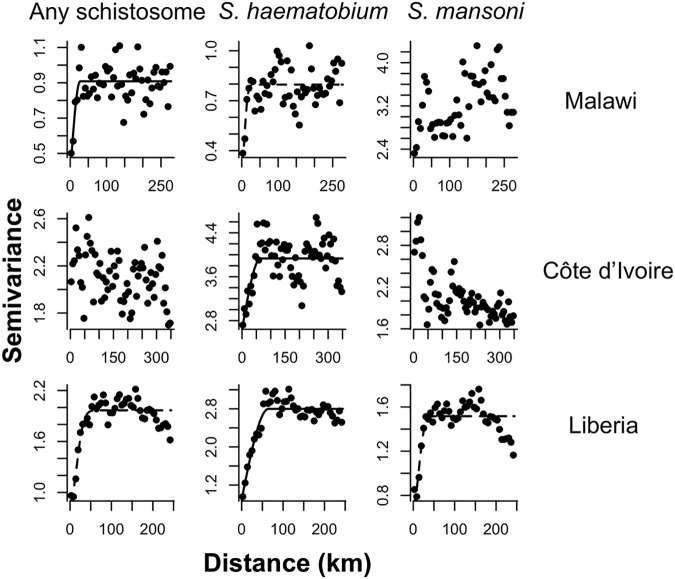
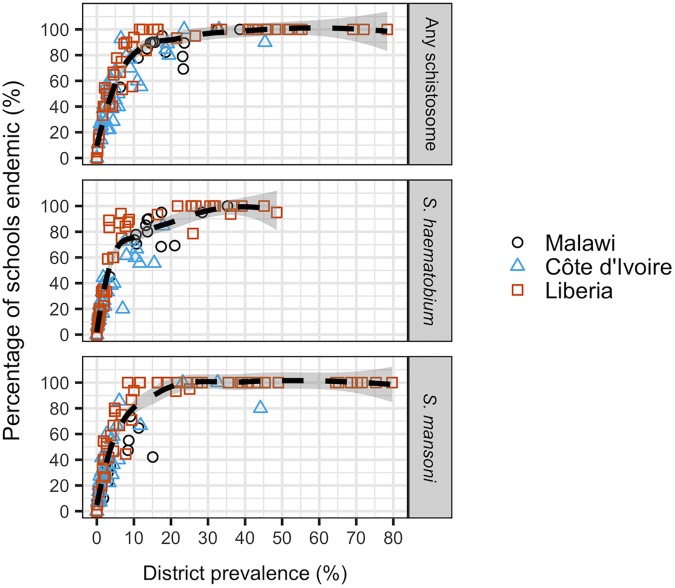
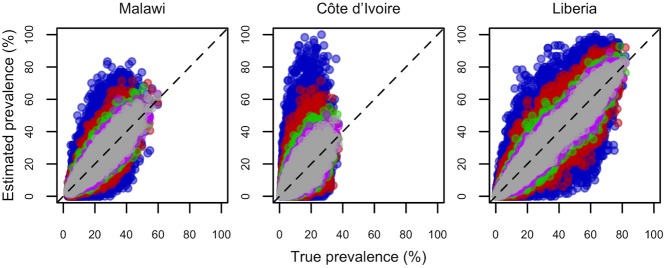
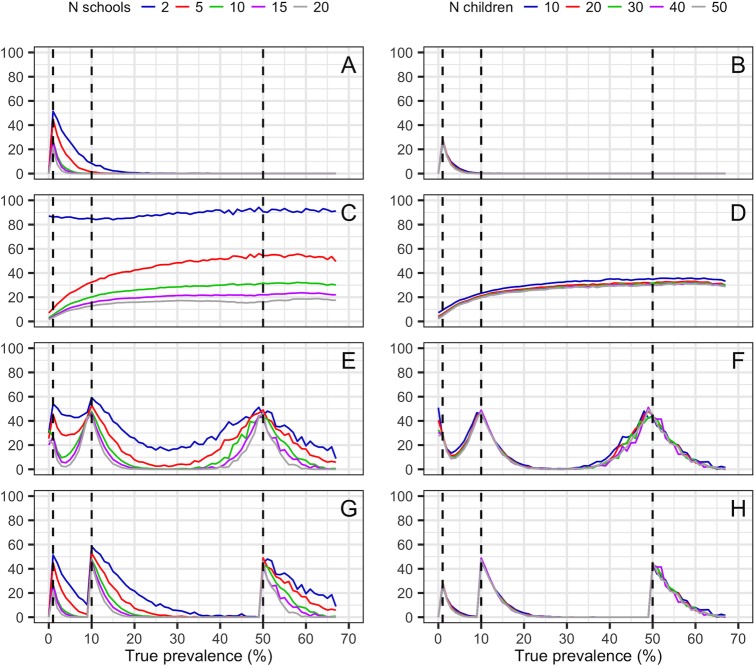
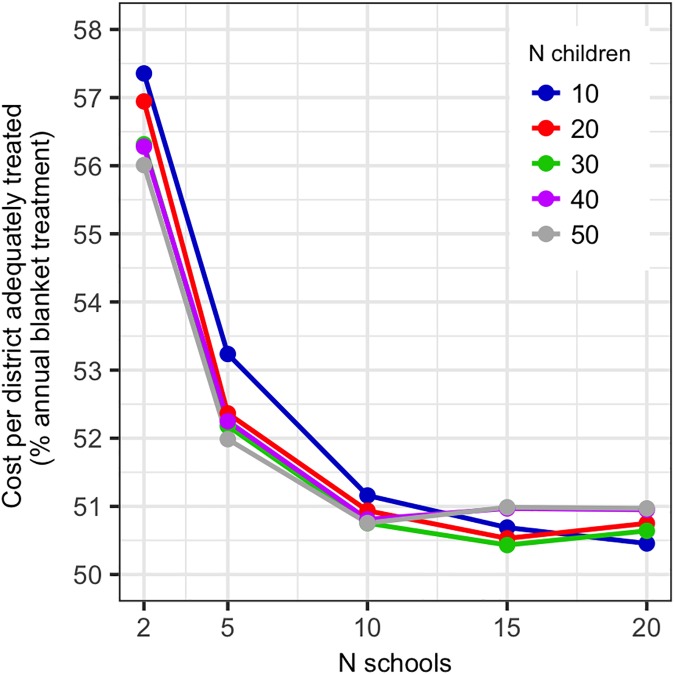
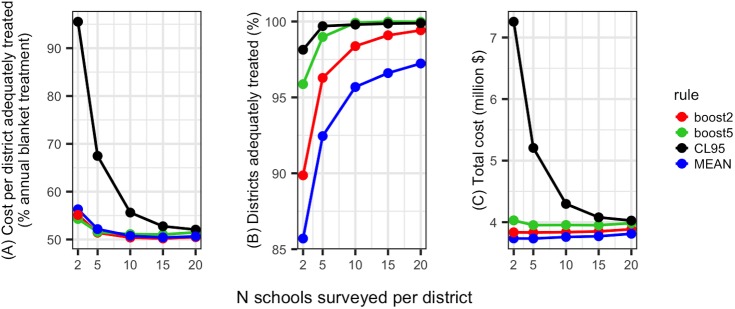
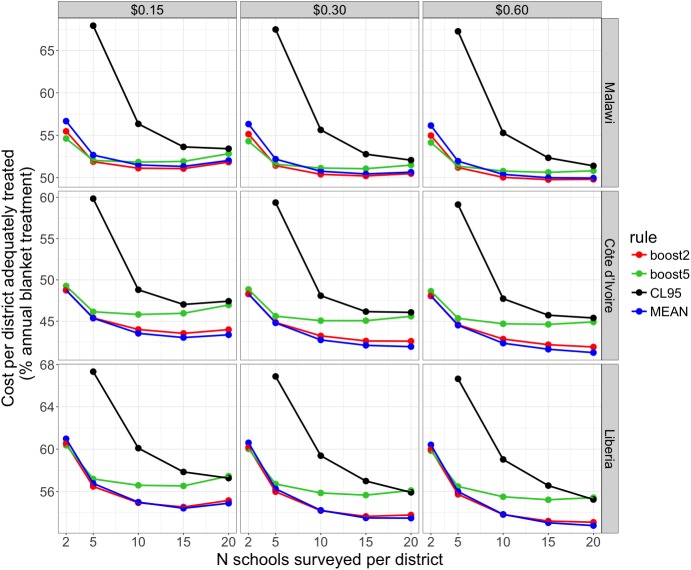
Methodology/principal findings: We used baseline schistosomiasis mapping surveys from three countries (Malawi, Côte d'Ivoire and Liberia) to generate spatially realistic gold standard datasets, against which we tested alternative two-stage cluster survey designs. We assessed how sampling different numbers of schools per district (2-20) and children per school (10-50) influences the accuracy of prevalence estimates and treatment class assignment, and we compared survey cost-efficiency using data from Malawi. Due to the focal nature of schistosomiasis, up to 53% simulated surveys involving 2-5 schools per district failed to detect schistosomiasis in low endemicity areas (1-10% prevalence). Increasing the number of schools surveyed per district improved treatment class assignment far more than increasing the number of children sampled per school. For Malawi, surveys of 15 schools per district and 20-30 children per school reliably detected endemic schistosomiasis and maximised cost-efficiency. In sensitivity analyses where treatment costs and the country considered were varied, optimal survey size was remarkably consistent, with cost-efficiency maximised at 15-20 schools per district.
Conclusions/significance: Among two-stage cluster surveys for schistosomiasis, our simulations indicated that surveying 15-20 schools per district and 20-30 children per school optimised cost-efficiency and minimised the risk of under-treatment, with surveys involving more schools of greater cost-efficiency as treatment costs rose.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Van Der Werf MJ, De Vlas SJ, Brooker S, Looman CWN, Nagelkerke NJD, Habbema JDF, et al. Quantification of clinical morbidity associated with schistosome infection in sub-Saharan Africa. Acta Trop. 2003;86: 125–139. - PubMed
-
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380: 2095–2128. doi: 10.1016/S0140-6736(12)61728-0 - DOI - PMC - PubMed
-
- Murray CJL, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380: 2197–2223. doi: 10.1016/S0140-6736(12)61689-4 - DOI - PubMed
-
- Fenwick A, Webster JP, Bosque-Oliva E, Blair L, Fleming FM, Zhang Y, et al. The Schistosomiasis Control Initiative (SCI): rationale, development and implementation from 2002–2008. Parasitology. 2009;136: 1719–30. doi: 10.1017/S0031182009990400 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
