

Cardioprotective Action of Ginkgo biloba Extract against Sustained β-Adrenergic Stimulation Occurs via Activation of M2/NO Pathway
- PMID: 28553225
- PMCID: PMC5426084
- DOI: 10.3389/fphar.2017.00220
Cardioprotective Action of Ginkgo biloba Extract against Sustained β-Adrenergic Stimulation Occurs via Activation of M2/NO Pathway
Abstract
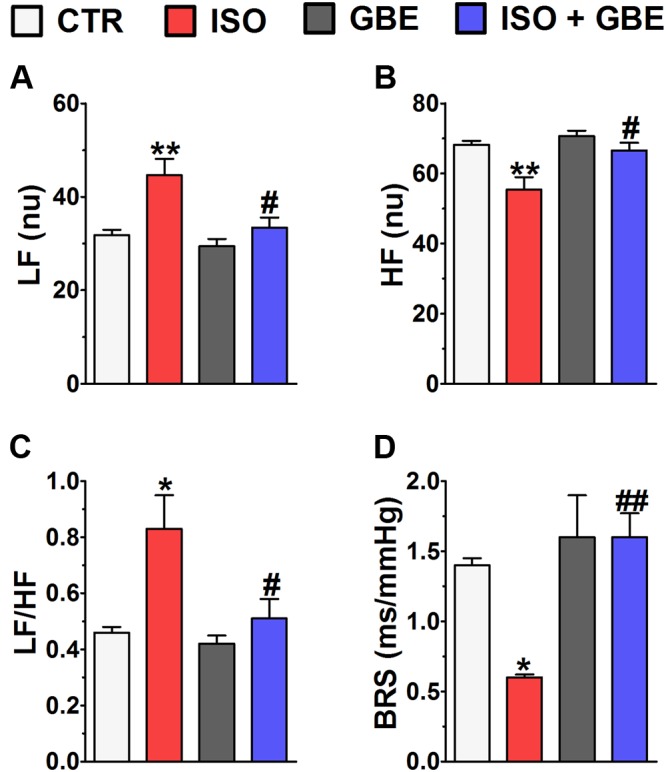
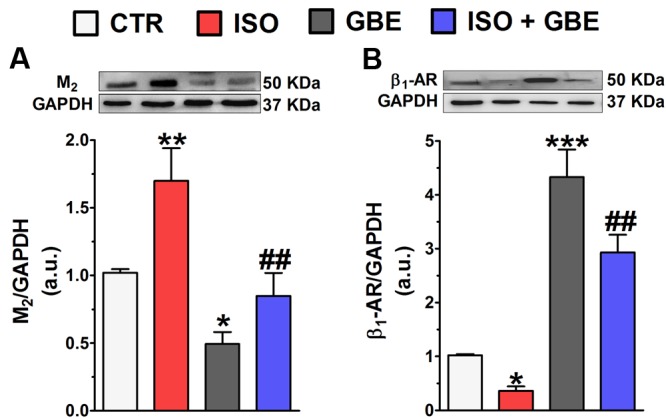
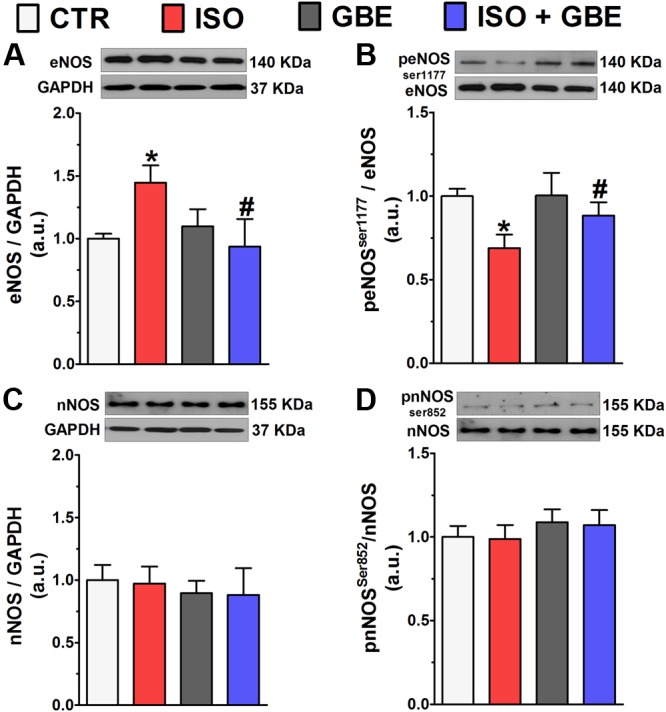
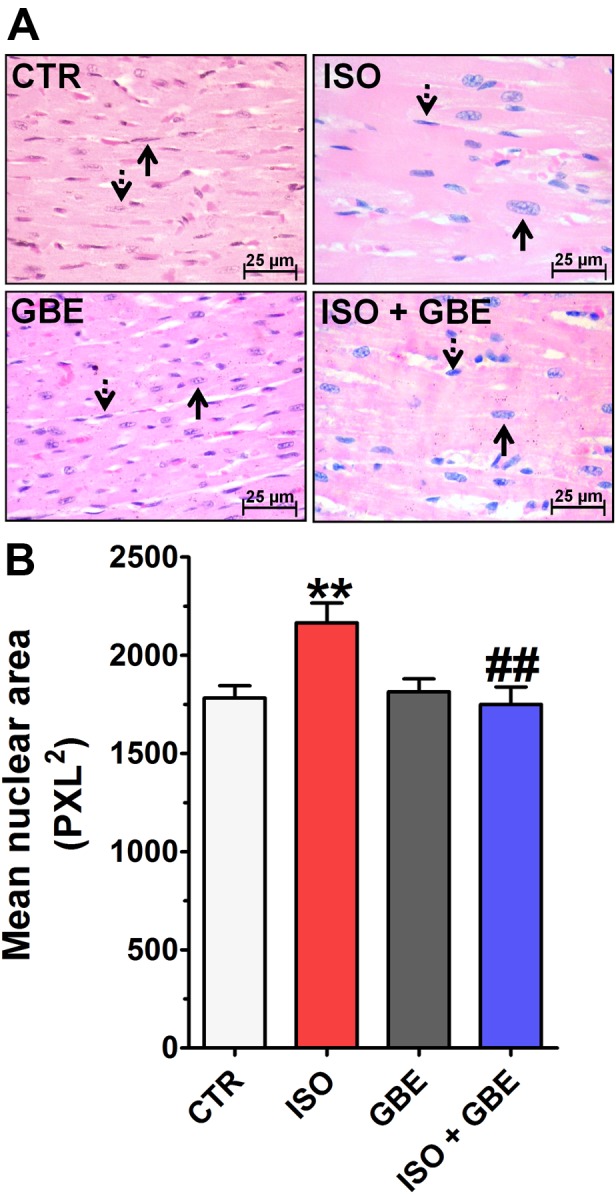
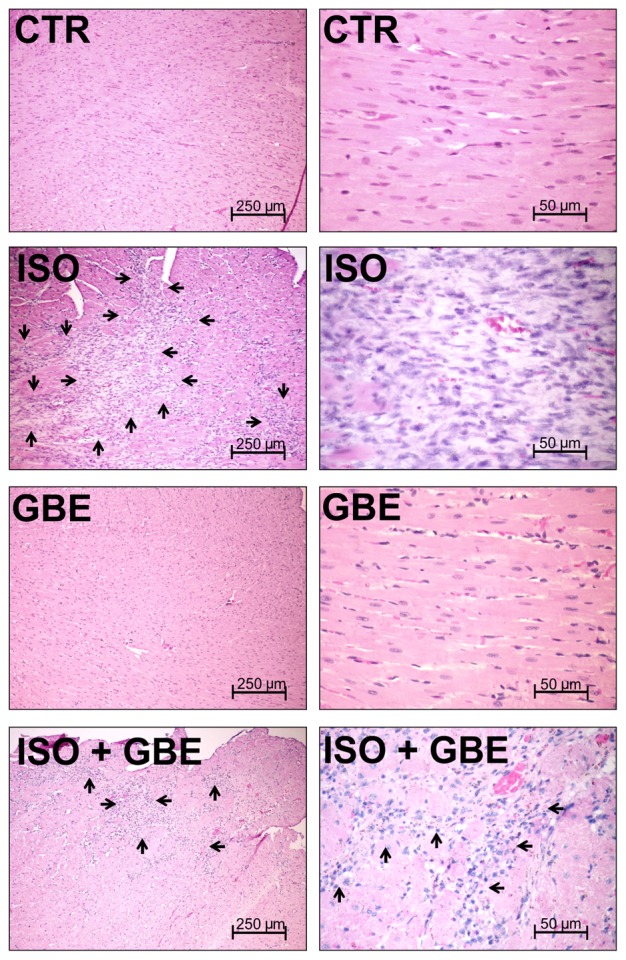
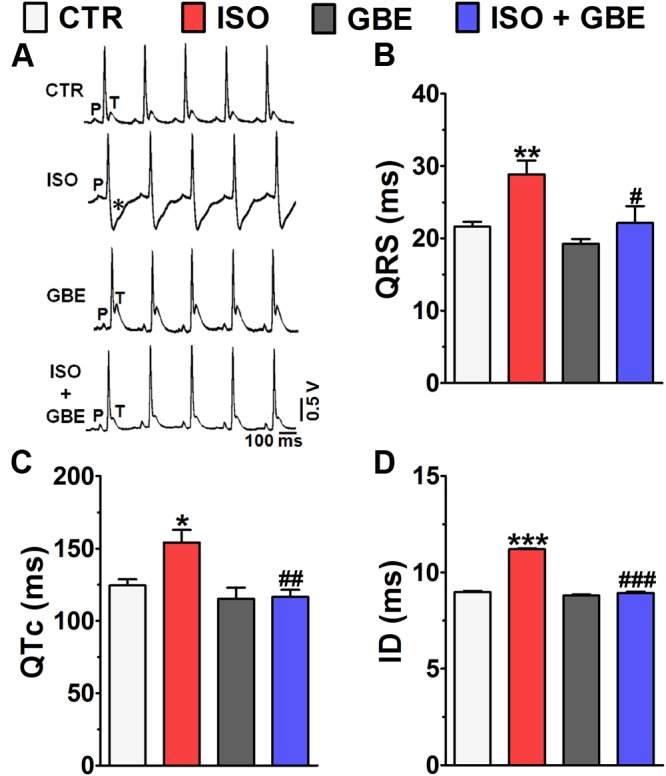
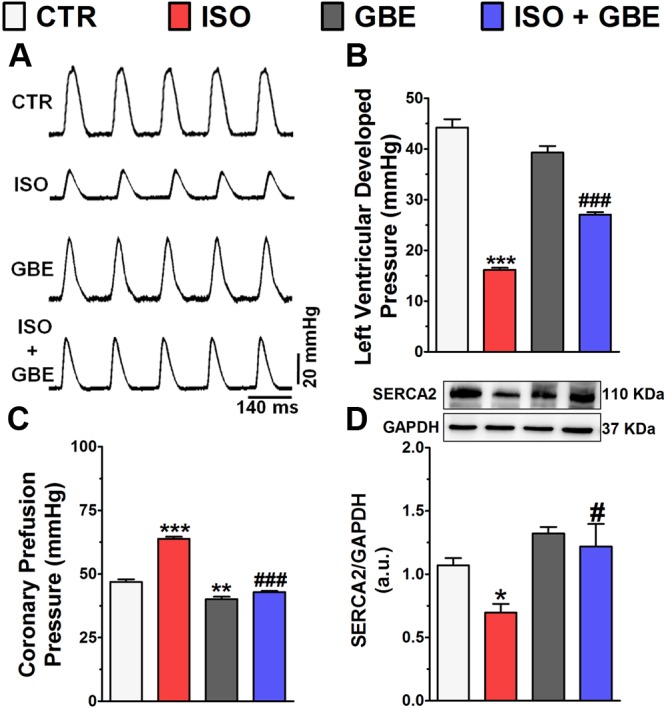
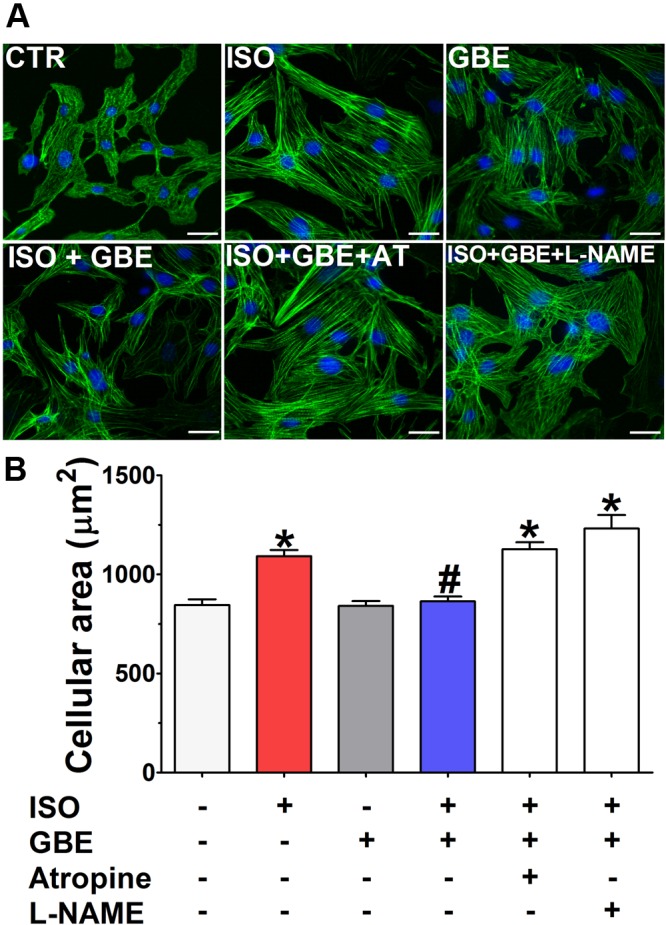
Ginkgo biloba is the most popular phytotherapic agent used worldwide for treatment of several human disorders. However, the mechanisms involved in the protective actions of Ginkgo biloba on cardiovascular diseases remain poorly elucidated. Taking into account recent studies showing beneficial actions of cholinergic signaling in the heart and the cholinergic hypothesis of Ginkgo biloba-mediated neuroprotection, we aimed to investigate whether Ginkgo biloba extract (GBE) promotes cardioprotection via activation of cholinergic signaling in a model of isoproterenol-induced cardiac hypertrophy. Here, we show that GBE treatment (100 mg/kg/day for 8 days, v.o.) reestablished the autonomic imbalance and baroreflex dysfunction caused by chronic β-adrenergic receptor stimulation (β-AR, 4.5 mg/kg/day for 8 days, i.p.). Moreover, GBE prevented the upregulation of muscarinic receptors (M2) and downregulation of β1-AR in isoproterenol treated-hearts. Additionally, we demonstrated that GBE prevents the impaired endothelial nitric oxide synthase activity in the heart. GBE also prevented the pathological cardiac remodeling, electrocardiographic changes and impaired left ventricular contractility that are typical of cardiac hypertrophy. To further investigate the mechanisms involved in GBE cardioprotection in vivo, we performed in vitro studies. By using neonatal cardiomyocyte culture we demonstrated that the antihypertrophic action of GBE was fully abolished by muscarinic receptor antagonist or NOS inhibition. Altogether, our data support the notion that antihypertrophic effect of GBE occurs via activation of M2/NO pathway uncovering a new mechanism involved in the cardioprotective action of Ginkgo biloba.
Keywords: Ginkgo biloba; cardiac hypertrophy; cholinergic signaling; chronic β-adrenergic stimulation; endothelial nitric oxide synthase.
Figures
Similar articles
-
Ginkgo biloba extract attenuates oxLDL-induced endothelial dysfunction via an AMPK-dependent mechanism.J Appl Physiol (1985). 2013 Jan 15;114(2):274-85. doi: 10.1152/japplphysiol.00367.2012. Epub 2012 Nov 29. J Appl Physiol (1985). 2013. PMID: 23195633
-
Ginkgo biloba extract inhibits oxidized low-density lipoprotein (oxLDL)-induced matrix metalloproteinase activation by the modulation of the lectin-like oxLDL receptor 1-regulated signaling pathway in human umbilical vein endothelial cells.J Vasc Surg. 2016 Jan;63(1):204-15.e1. doi: 10.1016/j.jvs.2014.05.098. Epub 2014 Jul 28. J Vasc Surg. 2016. PMID: 25080882
-
Ginkgo biloba L. extract protects against chronic cerebral hypoperfusion by modulating neuroinflammation and the cholinergic system.Phytomedicine. 2016 Nov 15;23(12):1356-1364. doi: 10.1016/j.phymed.2016.07.013. Epub 2016 Aug 1. Phytomedicine. 2016. PMID: 27765355
-
Ginkgo biloba Extract in Vascular Protection: Molecular Mechanisms and Clinical Applications.Curr Vasc Pharmacol. 2017;15(6):532-548. doi: 10.2174/1570161115666170713095545. Curr Vasc Pharmacol. 2017. PMID: 28707602 Review.
-
Clinical use and molecular mechanisms of action of extract of Ginkgo biloba leaves in cardiovascular diseases.Cardiovasc Drug Rev. 2004 Winter;22(4):309-19. doi: 10.1111/j.1527-3466.2004.tb00148.x. Cardiovasc Drug Rev. 2004. PMID: 15592576 Review.
Cited by
-
Inhibition of Myocardial Remodeling and Heart Failure by Traditional Herbal Medications: Evidence from Ginseng and ginkgo biloba.Rev Cardiovasc Med. 2023 Jul 21;24(7):212. doi: 10.31083/j.rcm2407212. eCollection 2023 Jul. Rev Cardiovasc Med. 2023. PMID: 39077021 Free PMC article. Review.
-
Noradrenaline Modulates the Membrane Potential and Holding Current of Medial Prefrontal Cortex Pyramidal Neurons via β1-Adrenergic Receptors and HCN Channels.Front Cell Neurosci. 2017 Nov 2;11:341. doi: 10.3389/fncel.2017.00341. eCollection 2017. Front Cell Neurosci. 2017. PMID: 29209170 Free PMC article.
-
A Systematic Review of Herbal Interventions for the Management of Cardiovascular Diseases.Curr Cardiol Rev. 2024;20(5):e030524229664. doi: 10.2174/011573403X286573240422104647. Curr Cardiol Rev. 2024. PMID: 38706368 Free PMC article.
-
Herbal Medicine for Cardiovascular Diseases: Efficacy, Mechanisms, and Safety.Front Pharmacol. 2020 Apr 7;11:422. doi: 10.3389/fphar.2020.00422. eCollection 2020. Front Pharmacol. 2020. PMID: 32317975 Free PMC article. Review.
-
A Comprehensive Review of Cardiovascular Disease Management: Cardiac Biomarkers, Imaging Modalities, Pharmacotherapy, Surgical Interventions, and Herbal Remedies.Cells. 2024 Sep 1;13(17):1471. doi: 10.3390/cells13171471. Cells. 2024. PMID: 39273041 Free PMC article. Review.
References
-
- Bertinieri G., di Rienzo M., Cavallazzi A., Ferrari A. U., Pedotti A., Mancia G. (1985). A new approach to analysis of the arterial baroreflex. J. Hypertens. Suppl. 3 S79–S81. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials